The Clinical Impact of Bedside Contrast Echocardiography in Intensive Care Settings: A Korean Multicenter Study
- Affiliations
-
- 1Department of Cardiology, Kyung Hee University School of Medicine, Seoul, Korea. issohn@khu.ac.kr
- 2Division of Cardiology, Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea.
- 3Division of Cardiology, Department of Internal Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 4Division of Cardiology, Heart Center, Gachon University Gil Hospital, Gachon University School of Medicine, Incheon, Korea.
- 5Division of Cardiology, Department of Internal Medicine, Pusan National University School of Medicine, Busan, Korea.
- 6Division of Cardiology, Department of Internal Medicine, Soonchunhyang University Hospital, Bucheon, Korea.
- 7Division of Cardiology, Department of Internal Medicine, NHIS Ilsan Hospital, Goyang, Korea.
- 8Division of Cardiology, Department of Internal Medicine, Kosin University Gospel Hospital, Busan, Korea.
- 9Division of Cardiology, Department of Internal Medicine, Keimyung University Dongsan Medical Center, Daegu, Korea.
- 10Division of Cardiology, Department of Internal Medicine, Chonnam National University Hospital, Gwangju, Korea.
- KMID: 2223787
- DOI: http://doi.org/10.4070/kcj.2015.45.6.486
Abstract
- BACKGROUND AND OBJECTIVES
We assessed the ability of portable echocardiography (with contrasts) to clearly delineate the cardiac structure, and evaluated the impact of its use on the diagnosis and management of critically ill patients in Korea.
SUBJECTS AND METHODS
We prospectively enrolled 123 patients (mean age 66+/-16 years), who underwent portable transthoracic echocardiography (with contrast) for image enhancement at 12 medical centers. The quality of the global left ventricular (LV) images, the number of the regional LV segments visualized, the ability to visualize the LV apex and the right ventricle (RV), and any changes in the diagnostic procedure and treatment strategy were compared before and after the contrast.
RESULTS
Of the 123 patients, 52 (42%) were using mechanical ventilators. The amount of poor or uninterpretable images decreased from 48% to 5% (p<0.001), after the contrast. Before the contrast, 15.6+/-1.1 of 16 LV segments were seen, which improved to 15.9+/-0.6 segments (p=0.001) after the contrast. The ability to visualize the LV apex increased from 47% to 94% (p<0.001), while the inability to clearly visualize the RV decreased from 46% to 19% (p<0.001). Changes in the diagnostic procedure (for example, not requiring other types of imaging studies) were observed in 18% of the patients, and the treatment plan (medication) was altered in 26% of patients after the contrast echocardiography.
CONCLUSION
The use of a contrast agent during the portable echocardiography, in intensive care settings, can improve the image quality and impact the diagnostic procedures and treatment for Korean patients.
Keyword
MeSH Terms
Figure
-
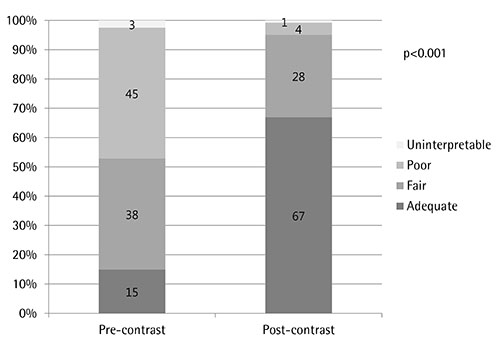
Fig. 1 The effect of contrast echocardiography on the global left ventricular (LV) image quality. Contrast echocardiography significantly improves the general LV image quality, compared to fundamental echocardiography (McNemar's test, p<0.001 comparing uninterpretable and poor with fair and adequate).
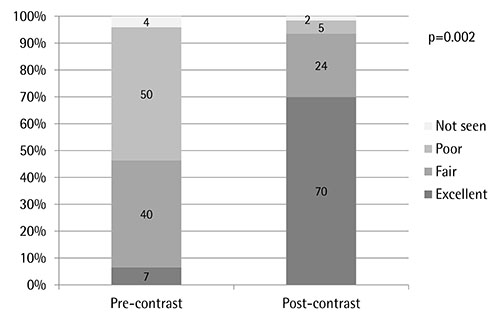
Fig. 2 The effect of contrast echocardiography on the visualization of the left ventricular (LV) apex. Contrast echocardiography significantly improves the ability to visualize the LV apex, compared to fundamental echocardiography (p<0.001).

Fig. 3 The effect of contrast echocardiography on the visualization of the right ventricle (RV). Contrast echocardiography significantly improves the ability to visualize the RV (p<0.001).
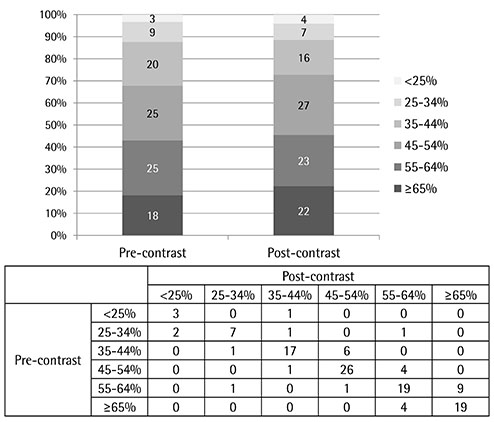
Fig. 4 A comparison of the estimated ejection fractions, between pre-contrast and post-contrast images (Wilcoxon signed rank test, p=0.106, in incremental ranges of 10%).

Fig. 5 The impact of contrast echocardiography on diagnostic procedures. Contrast echocardiography decreased the need for additional diagnostic imaging procedures in 22 patients (18%). TEE: transesophageal echocardiography, CAG: coronary angiography.
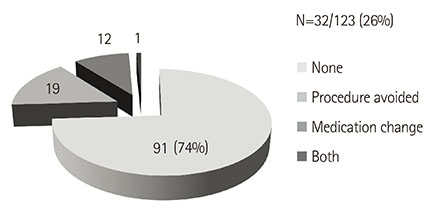
Fig. 6 The impact of contrast echocardiography on management strategies. Contrast echocardiography altered the management plan for 32 patients (26%).
Reference
-
1. Beaulieu Y. Bedside echocardiography in the assessment of the critically ill. Crit Care Med. 2007; 35:5 Suppl. S235–S249.2. Senior R, Dwivedi G, Hayat S, Lim TK. Clinical benefits of contrast-enhanced echocardiography during rest and stress examinations. Eur J Echocardiogr. 2005; 6:Suppl 2. S6–S13.3. Hwang JJ, Shyu KG, Chen JJ, Tseng YZ, Kuan P, Lien WP. Usefulness of transesophageal echocardiography in the treatment of critically ill patients. Chest. 1993; 104:861–866.4. Cook CH, Praba AC, Beery PR, Martin LC. Transthoracic echocardiography is not cost-effective in critically ill surgical patients. J Trauma. 2002; 52:280–284.5. Senior R, Becher H, Monaghan M, et al. Contrast echocardiography: evidence-based recommendations by European Association of Echocardiography. Eur J Echocardiogr. 2009; 10:194–212.6. Hundley WG, Kizilbash AM, Afridi I, Franco F, Peshock RM, Grayburn PA. Administration of an intravenous perfluorocarbon contrast agent improves echocardiographic determination of left ventricular volumes and ejection fraction: comparison with cine magnetic resonance imaging. J Am Coll Cardiol. 1998; 32:1426–1432.7. Hundley WG, Kizilbash AM, Afridi I, Franco F, Peshock RM, Grayburn PA. Effect of contrast enhancement on transthoracic echocardiographic assessment of left ventricular regional wall motion. Am J Cardiol. 1999; 84:1365–1368. A8–A9.8. Kurt M, Shaikh KA, Peterson L, et al. Impact of contrast echocardiography on evaluation of ventricular function and clinical management in a large prospective cohort. J Am Coll Cardiol. 2009; 53:802–810.9. Reilly JP, Tunick PA, Timmermans RJ, Stein B, Rosenzweig BP, Kronzon I. Contrast echocardiography clarifies uninterpretable wall motion in intensive care unit patients. J Am Coll Cardiol. 2000; 35:485–490.10. Makaryus AN, Zubrow ME, Gillam LD, et al. Contrast echocardiography improves the diagnostic yield of transthoracic studies performed in the intensive care setting by novice sonographers. J Am Soc Echocardiogr. 2005; 18:475–480.11. Yong Y, Wu D, Fernandes V, et al. Diagnostic accuracy and cost-effectiveness of contrast echocardiography on evaluation of cardiac function in technically very difficult patients in the intensive care unit. Am J Cardiol. 2002; 89:711–718.12. Jung HO. Pericardial effusion and pericardiocentesis: role of echocardiography. Korean Circ J. 2012; 42:725–734.13. Mulvagh SL, Rakowski H, Vannan MA, et al. American Society of Echocardiography Consensus Statement on the clinical applications of ultrasonic contrast agents in echocardiography. J Am Soc Echocardiogr. 2008; 21:1179–1201. quiz 128114. Lang RM, Bierig M, Devereux RB, et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography's Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005; 18:1440–1463.15. Mulvagh SL, DeMaria AN, Feinstein SB, et al. Contrast echocardiography: current and future applications. J Am Soc Echocardiogr. 2000; 13:331–342.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Persistent left superior vena cava: diagnosed by bedside echocardiography in a liver transplant patient: a case report
- Transthoracic echocardiography probe in an anesthesiologist's hand: utility in the operating room
- Impact of 8-Week Bedside Ultrasound Training for Surgical Residents in the Intensive Care Unit of a Tertiary Care Hospital - a Pilot Study
- Bedside ultrasound-guided percutaneous cystostomy in an infant in the neonatal intensive care unit
- A Primer on the Methods and Applications for Contrast Echocardiography in Clinical Imaging
