J Rheum Dis.
2015 Aug;22(4):260-262. 10.4078/jrd.2015.22.4.260.
A Case of Bad Prognosis for Membranous Nephropathy in a Patient with Mixed Connective Tissue Disease
- Affiliations
-
- 1Division of Nephrology, Inje University Seoul Paik Hospital, Inje University College of Medicine, Seoul, Korea. hoseok.koo@gmail.com
- 2Department of Internal Medicine, Inje University Seoul Paik Hospital, Inje University College of Medicine, Seoul, Korea.
- KMID: 2222859
- DOI: http://doi.org/10.4078/jrd.2015.22.4.260
Abstract
- Incidence of renal involvement in mixed connective tissue disease (MCTD) is low. In the presence of glomerulonephritis, membranous nephropathy (MN) in MCTD is common. A 47-year-old woman presented with hypothyroidism. She developed Raynaud's phenomenon, arthralgia, and incomplete lupus erythematosus, diagnosed with MCTD. One year after then, the patient developed persistent proteinuria (1+) without hematuria. Following diagnosis with MCTD, her renal function began to deteriorate. The renal biopsy showed late stage MN. For the treatment of MN with mild proteinuria and MCTD, we prescribed an angiotensin II receptor blocker and 7.5 mg of methotrexate per week and 300 mg of hydroxychloroquine daily. The patient had a reduced estimated glomerular filtration rate of 55% for the subsequent eight years. The MN in MCTD is known to show good renal prognosis. Here, we report on a rare case of MN in MCTD in Korea with a bad prognosis.
MeSH Terms
-
Arthralgia
Biopsy
Diagnosis
Female
Glomerular Filtration Rate
Glomerulonephritis
Glomerulonephritis, Membranous*
Hematuria
Humans
Hydroxychloroquine
Hypothyroidism
Incidence
Korea
Methotrexate
Middle Aged
Mixed Connective Tissue Disease*
Prognosis*
Proteinuria
Receptors, Angiotensin
Hydroxychloroquine
Methotrexate
Receptors, Angiotensin
Figure
-
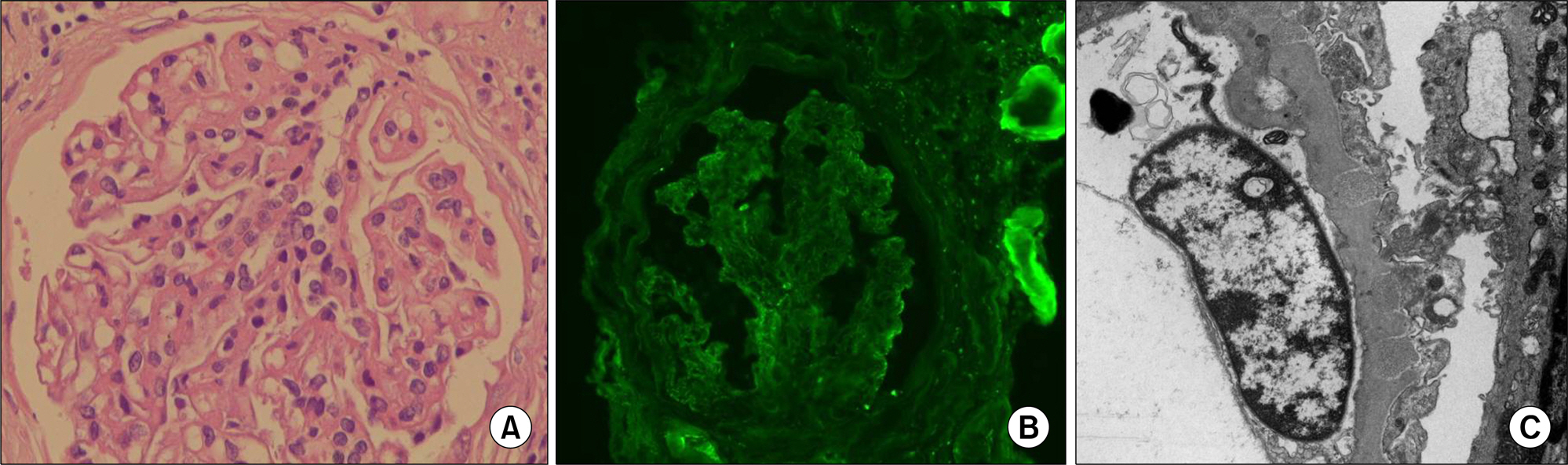
Figure 1. (A) Glomeruli sclerosis of 23.1% involves mesangial cells and endothelial cells (H&E, ×400). (B) Immunoglobulin G was slightly stained in the periphery (IF, ×400). (C) Electron-dense deposits were in some subepithelial and intramembranous deposits. The diffuse effacement of podocyte foot process and a dome and spike formation were evident (EM, ×10,000).
Reference
-
1. Sharp GC, Irvin WS, Tan EM, Gould RG, Holman HR. Mixed connective tissue disease: an apparently distinct rheumatic disease syndrome associated with a specific anti-body to an extractable nuclear antigen (ENA). Am J Med. 1972; 52:148–59.2. Aringer M, Smolen JS. Mixed connective tissue disease: what is behind the curtain? Best Pract Res Clin Rheumatol. 2007; 21:1037–49.
Article3. Sharp GC, Irvin WS, May CM, Holman HR, McDuffie FC, Hess EV, et al. Association of antibodies to ribonucleoprotein and Sm antigens with mixed connective-tissue disease, systematic lupus erythematosus and other rheumatic diseases. N Engl J Med. 1976; 295:1149–54.4. Pope JE. Other manifestations of mixed connective tissue disease. Rheum Dis Clin North Am. 2005; 31:519–33.
Article5. Burdt MA, Hoffman RW, Deutscher SL, Wang GS, Johnson JC, Sharp GC. Long-term outcome in mixed connective tissue disease: longitudinal clinical and serologic findings. Arthritis Rheum. 1999; 42:899–909.
Article6. Kitridou RC, Akmal M, Turkel SB, Ehresmann GR, Quismorio FP Jr, Massry SG. Renal involvement in mixed connective tissue disease: a longitudinal clinicopathologic study. Semin Arthritis Rheum. 1986; 16:135–45.
Article7. Alarcón-Segovia D, Cardiel MH. Comparison between 3 diagnostic criteria for mixed connective tissue disease. Study of 593 patients. J Rheumatol. 1989; 16:328–34.8. Radford MG Jr, Holley KE, Grande JP, Larson TS, Wagoner RD, Donadio JV, et al. Reversible membranous nephropathy associated with the use of nonsteroidal anti-inflammatory drugs. JAMA. 1996; 276:466–9.
Article9. Schieppati A, Mosconi L, Perna A, Mecca G, Bertani T, Garattini S, et al. Prognosis of untreated patients with idiopathic membranous nephropathy. N Engl J Med. 1993; 329:85–9.
Article10. Reichert LJ, Koene RA, Wetzels JF. Prognostic factors in idiopathic membranous nephropathy. Am J Kidney Dis. 1998; 31:1–11.
Article11. McLeish KR, Smith MR, Gohara AF. Non-Hodgkin's lymphoma and membranous nephropathy in mixed connective tissue disease. Am J Med Sci. 1985; 290:152–4.12. Kobayashi S, Nagase M, Kimura M, Ohyama K, Ikeya M, Honda N. Renal involvement in mixed connective tissue disease. Report of 5 cases. Am J Nephrol. 1985; 5:282–9.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case presentation of renal involvement in MCTD
- A Case of Trigeminal Neuropathy Associated with Mixed Connective Tissue Disease
- A case of membranous nephropathy associated with relapsing polychondritis
- A Case of IgA Nephropathy Associated with Early Gastric Cancer
- Adult Onset Still's Disease Developed in a Patient with Membranous Nephropathy Treated with Immunosuppressive Agent
