A Case of Acute Calcium Pyrophosphate Crystal Arthritis in the Lumbar Facet Joint
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam, Korea. yn35@snu.ac.kr
- 2Department of Internal Medicine, Kangdong Sacred Heart Hospital, Seoul, Korea.
- 3Department of Radiology, Seoul National University Bundang Hospital, Seongnam, Korea.
- 4Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2222790
- DOI: http://doi.org/10.4078/jrd.2016.23.2.125
Abstract
- Calcium pyrophosphate dihydrate deposition disease most commonly presents with acute arthritis of the peripheral joints. Infrequently, a mass effect of this disease can cause axial symptoms, such as spinal stenosis, radiculopathy, or myelopathy. Herein, we report on the first Korean case of acute arthritis in the lumbar facet joint due to calcium pyrophosphate dihydrate crystal deposition disease. A 73-year-old female presented with acute fever, severe lumbago, and knee arthralgia, 11 days after partial parathyroidectomy. Plain radiographs showed multiple chondrocalcinosis, while a bone scan, computed tomography, and magnetic resonance imaging showed right L5-S1 facet arthritis. In synovial fluid from the facet and knee joints, positively birefringent calcium pyrophosphate dihydrate crystals were observed under polarized light microscopy. Under the diagnosis of acute calcium pyrophosphate dihydrate crystal arthritis (formerly known as 'pseudogout') in the facet joint, an intra-articular triamcinolone injection was administered, which resulted in dramatic improvement of the symptoms within 24 hours.
Keyword
MeSH Terms
-
Aged
Arthralgia
Arthritis*
Calcium Pyrophosphate*
Calcium*
Chondrocalcinosis
Diagnosis
Female
Fever
Humans
Joints
Knee
Knee Joint
Low Back Pain
Magnetic Resonance Imaging
Microscopy, Polarization
Parathyroidectomy
Radiculopathy
Spinal Cord Diseases
Spinal Stenosis
Synovial Fluid
Triamcinolone
Zygapophyseal Joint*
Calcium
Calcium Pyrophosphate
Triamcinolone
Figure
-
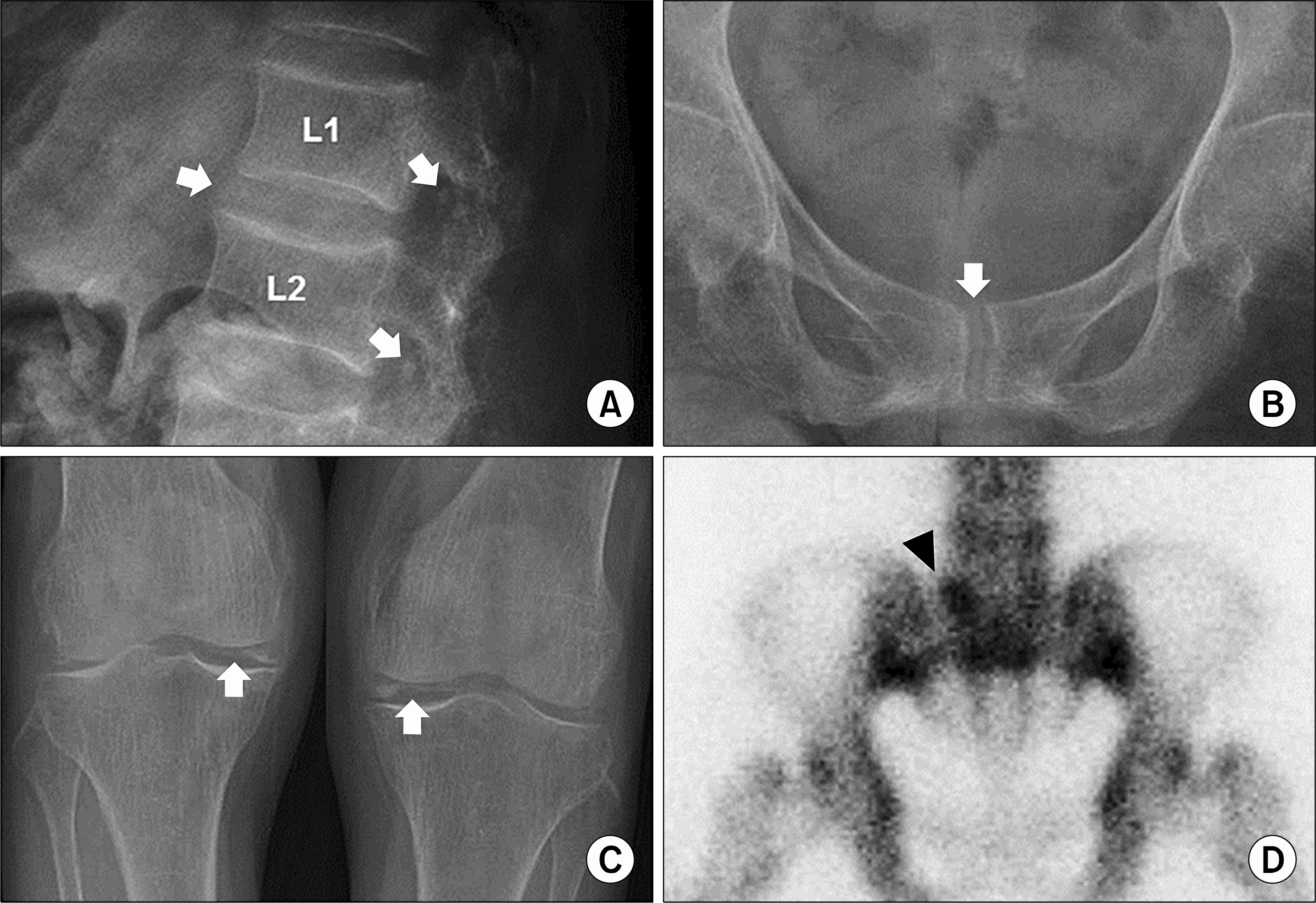
Figure 1. Plain radiographs and bone scan. Radiographs show calcification (white arrows) in the intervertebral and foraminal spaces (A), pubic symphysis (B), and meniscus (C). (D) A technetium bone scan demonstrates increased radiotracer uptake in the right L5-S1 facet joint (black arrowhead).
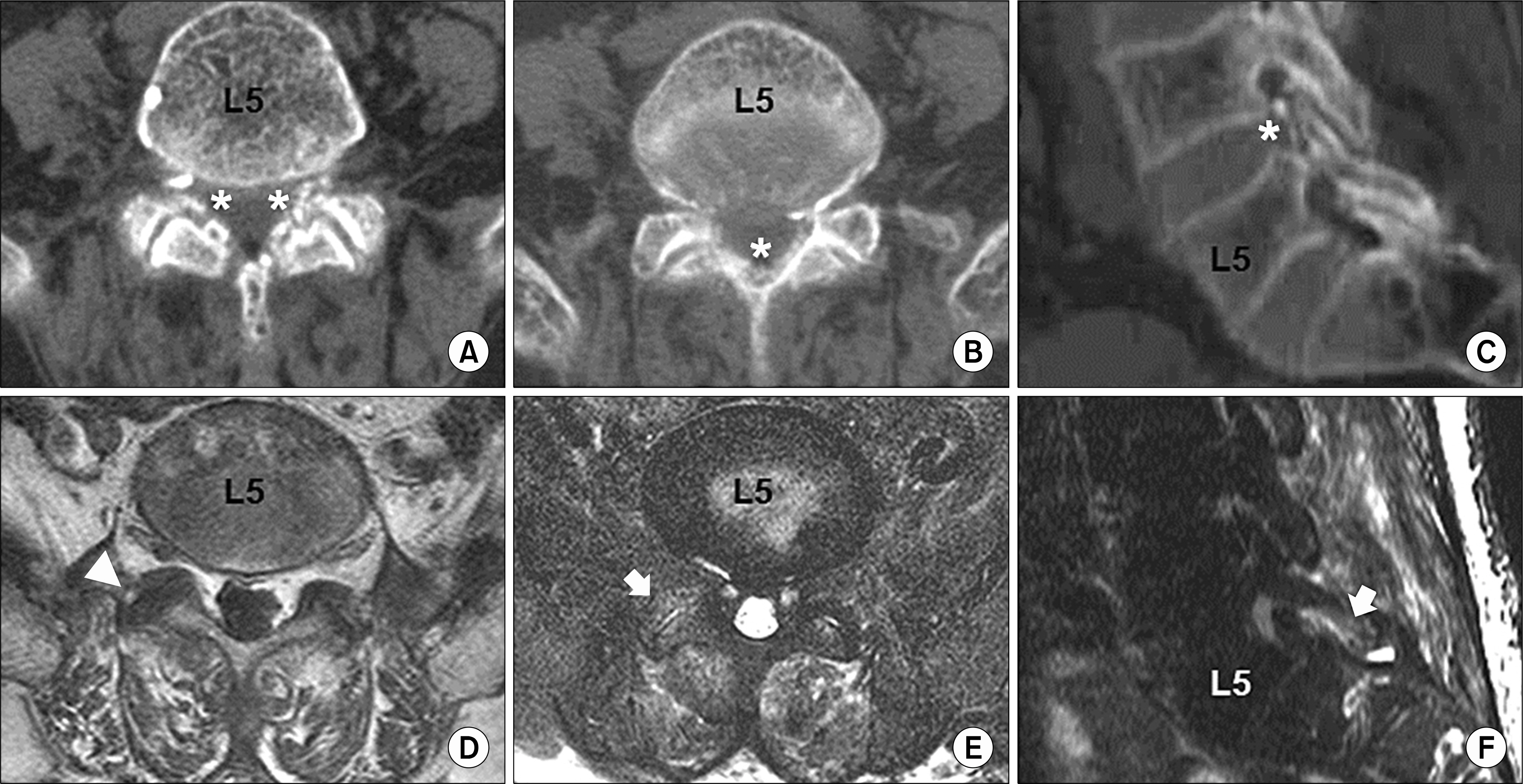
Figure 2. Lumbar spine computed tomography scans and magnetic resonance images. (A∼ C) Axial and sagittal computed tomography scans show calcification of the L5-S1 facet joint capsules, ligamentum flavum, and annulus fibrosus (asterisks). (D) Calcification around the facet joint is demonstrated as low signal intensity on a T1-weighted magnetic resonance image (white ar-rowhead). (E, F) T2-weighted and fat-suppressed imaging reveals facet joint effusion and bone marrow edema (white arrows).

Figure 3. Compensated polarized light microscopy of a synovial fluid sample from the facet joint. Intracellular calcium pyrophosphate dihydrate crystals appear as rhomboids with positive birefringence (×200). The double headed arrows indicate the axis of the analyzer.
Reference
-
1. Zhang W, Doherty M, Bardin T, Barskova V, Guerne PA, Jansen TL, et al. European League Against Rheumatism recommendations for calcium pyrophosphate deposition. Part I: terminology and diagnosis. Ann Rheum Dis. 2011; 70:563–70.
Article2. Ea HK, Lioté F. Diagnosis and clinical manifestations of calcium pyrophosphate and basic calcium phosphate crystal deposition diseases. Rheum Dis Clin North Am. 2014; 40:207–29.
Article3. Bong D, Bennett R. Pseudogout mimicking systemic disease. JAMA. 1981; 246:1438–40.
Article4. Grobost V, Vayssade M, Roche A, Kemeny JL, Soubrier M. Axial calcium pyrophosphate dihydrate deposition disease revealed by recurrent sterile spondylodiscitis and epidural abscess. Joint Bone Spine. 2014; 81:180–2.
Article5. Mikhael MM, Chioffe MA, Shapiro GS. Calcium pyrophosphate dihydrate crystal deposition disease (pseudogout) of lumbar spine mimicking osteomyelitis-discitis with epidural phlegmon. Am J Orthop (Belle Mead NJ). 2013; 42:E64–7.6. Ogawa Y, Nagatsuma M, Kubota G, Inoue G, Eguchi Y, Orita S, et al. Acute lumbar spinal pseudogout attack after instrumented surgery. Spine (Phila Pa 1976). 2012; 37:E1529–33.
Article7. Ziadé M, Zufferey P, So AK. Recurrent acute low back pain secondary to lumbar epidural calcification. Skeletal Radiol. 2007; 36(Suppl 1):S116–9.
Article8. Cameron CR, Burgess CD. Recurrent back pain and fevers. Med J Aust. 2007; 186:208–9.
Article9. Bartlett CS 3rd, Casden AM, Abdelwahab IF. Calcium pyrophosphate deposition disease mimicking infection in the lumbar spine. Orthopedics. 1999; 22:79–81.
Article10. Fujishiro T, Nabeshima Y, Yasui S, Fujita I, Yoshiya S, Fujii H. Pseudogout attack of the lumbar facet joint: a case report. Spine (Phila Pa 1976). 2002; 27:E396–8.
Article11. Wendling D, Martin M, Guillot X, Prati C. Interspinous bursitis and chondrocalcinosis. Joint Bone Spine. 2012; 79:516.
Article12. Lam HY, Cheung KY, Law SW, Fung KY. Crystal arthropathy of the lumbar spine: a report of 4 cases. J Orthop Surg (Hong Kong). 2007; 15:94–101.
Article13. Sekijima Y, Yoshida T, Ikeda S. CPPD crystal deposition disease of the cervical spine: a common cause of acute neck pain encountered in the neurology department. J Neurol Sci. 2010; 296:79–82.
Article14. Jeon CH, Choe WH, Ahn JK, Koh JH, Cha HS, Ahn JM, et al. Calcium pyrophosphate dihydrate (CPPD) crystal deposition disease mimicking meningitis: a case report and review of the literature. J Korean Rheum Assoc. 2001; 8:134–9.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of CPPD Crystal Deposition Disease in a Patient with Rheumatoid Arthritis and Systemic Sclerosis
- A Case of Calcium Pyrophosphate Dihydrate Crystal Deposition Disease Presenting as an Acute Polyarthritis
- Calcium pyrophosphate dehydrate crystal deposition disease of knee joint: a case report
- Calcium Pyrophosphate Dihydrate (CPPD)Crystal Deposition Disease Mimicking Meningitis:A case Report and Review of the Literature
- Prominent Inflammatory Features of Monocytes/Macrophages in Acute Calcium Pyrophosphate Crystal Arthritis: a Comparison with Acute Gouty Arthritis
