A Case of Wegener's Granulomatosis with Central Nervous System Involvement Mimicking Lung Cancer with Brain Metastasis
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Korea University Ansan Hospital, Ansan, Korea. csjmd@hotmail.com
- 2Division of Rheumatology, Department of Internal Medicine, Korea University Anam Hospital, Seoul, Korea.
- 3Division of Rheumatology, Department of Internal Medicine, Korea University Guro Hospital, Seoul, Korea.
- 4Department of Internal Medicine, Korea University Anam Hospital, Seoul, Korea.
- KMID: 2222758
- DOI: http://doi.org/10.4078/jrd.2013.20.3.181
Abstract
- Wegener's granulomatosis (WG) classically consists of necrotizing granulomatous inflammation of the upper and/or lower respiratory tract, necrotizing glomerulonephritis, and an autoimmune necrotizing systemic vasculitis affecting predominantly small vessels. We report a case of WG with central nervous system (CNS) involvement. WG is being diagnosed through pulmonary nodule biopsy. A small nodular lesion in the left posterior basal ganglia of brain being highly suspicious for granulomatosis was detected by MRI. After IV pulse cyclophosphamide and oral corticosteroid treatment for over 4 months, clinical manifestations and CNS lesions in brain MRI is improved. WG might have multiple granulomatous lesions which could be misdiagnosed due to malignancy. CNS involvement in WG is rare but careful evaluation is necessary when there are suspicious symptoms or lesions in CNS.
Keyword
MeSH Terms
Figure
-

Figure 1. Chest X ray (PA and lateral view) shows nodular opa-cities and cavitary lesions in both upper lung fields and patchy opa-cities in both lower lung fields.

Figure 2. Chest CT shows multiple cavities and nodules in both lung fields and focal consolidation is also noted in upper right lobe.
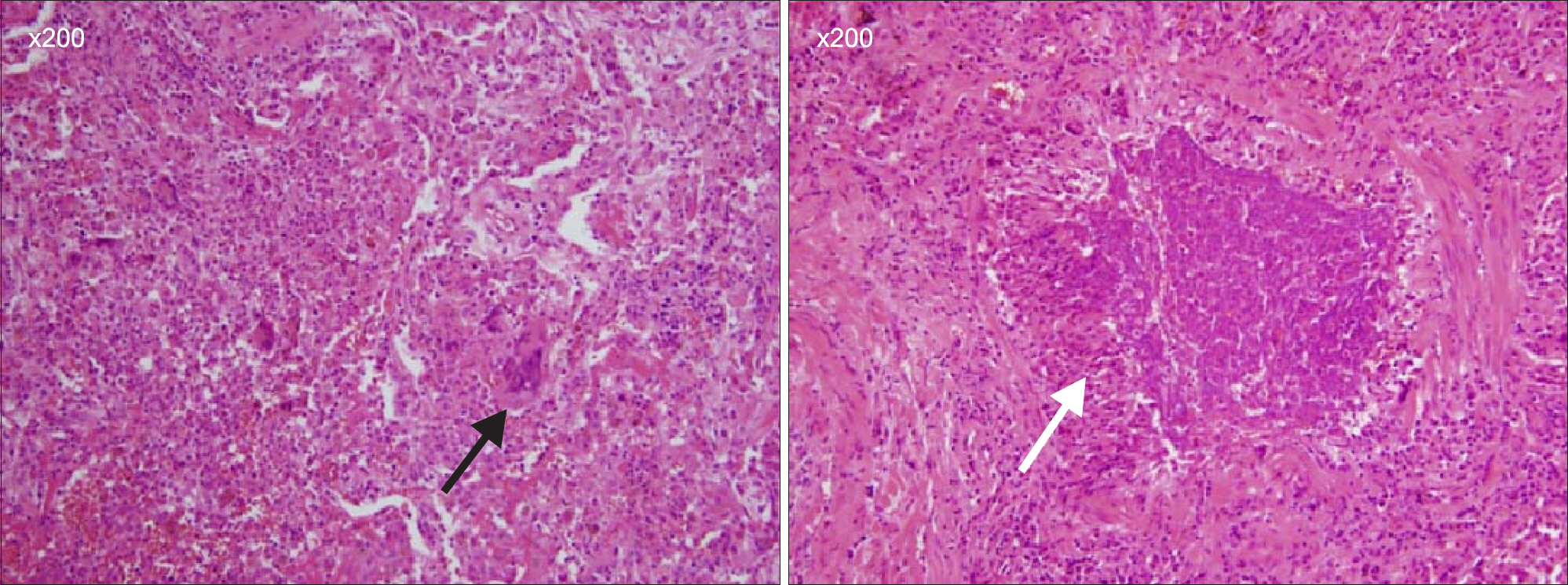
Figure 3. Hematoxylin and eosin stain of a lung nodule. Tissue obtained from VATS biopsy showed giant cells (black arrow) and necrotizing granulomatous vasculitis (white arrow).
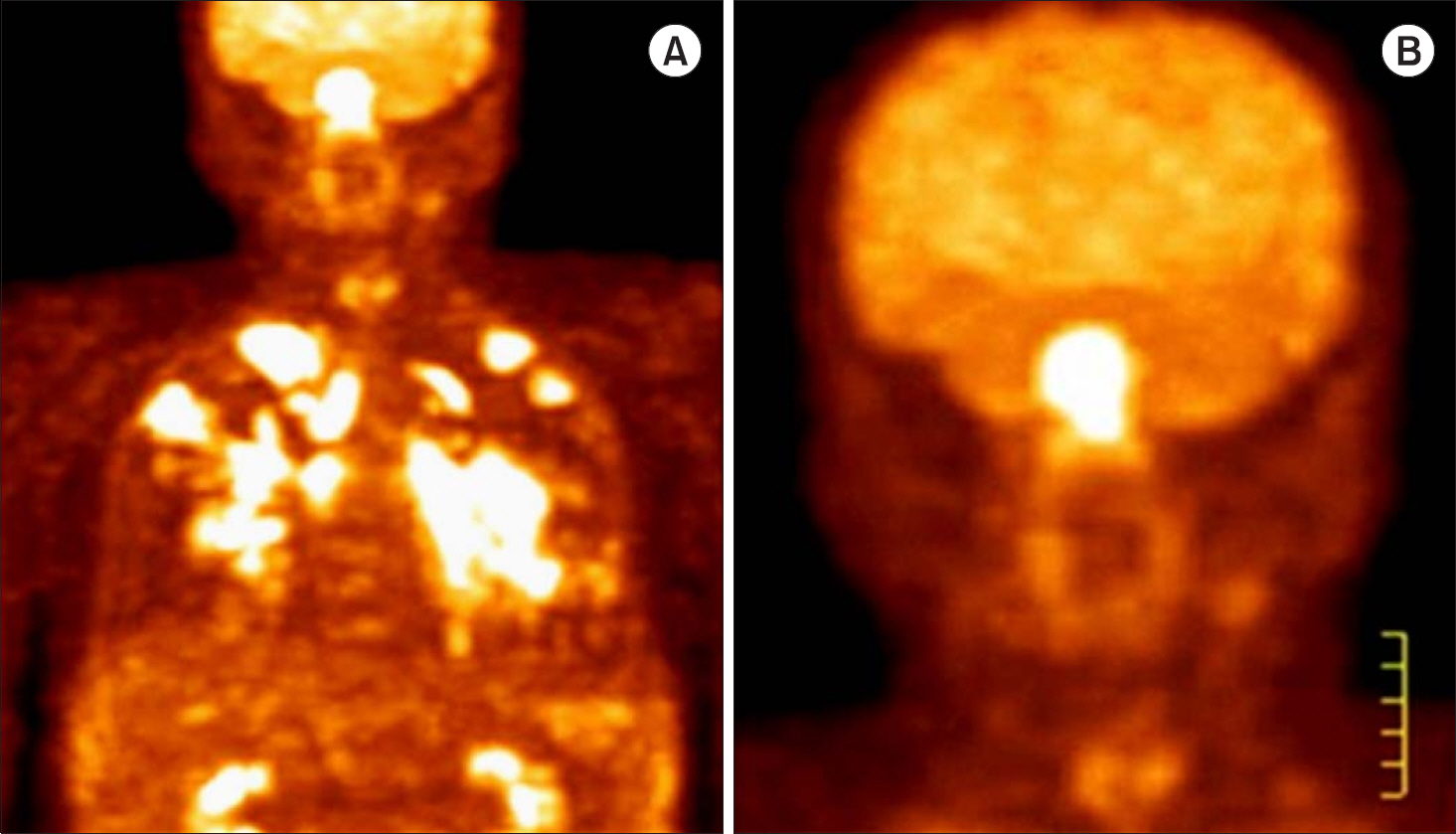
Figure 4. 18FDG PET-CT (A) Multiple hyper-metabolic lesions in the nasal septum and in both lungs with similar metabolisms (B) Multiple hyper-metabolic lesions in the nasal septum with extension into the adjacent nasal mucosa with similar metabolisms to those of the lungs.18 FDG PET-CT (A)

Figure 5. T1-enhanced MR images before (A, C) and after (B, D) four times cyclophosphamide pulse therapy. Arrow indicates an 8.2 mm- sized rim-enhancing small nodule in the left posterior basal ganglia mimicking metastatic cancer.
Reference
-
References
1. Schilder AM. Wegener's Granulomatosis vasculitis and granuloma. Autoimmun Rev. 2010; 9:483–7.
Article2. Lamprecht P, Gross WL. Wegener's granulomatosis. Herz. 2004; 29:47–56.
Article3. Zhang W, Zhou G, Shi Q, Zhang X, Zeng XF, Zhang FC. Clinical analysis of nervous system involvement in ANCA-associated systemic vasculitides. Clin Exp Rheumatol. 2009; 27(1 Suppl 52):S65–9.4. Nishino H, Rubino FA, DeRemee RA, Swanson JW, Parisi JE. Neurological involvement in Wegener's granulomatosis: an analysis of 324 consecutive patients at the Mayo Clinic. Ann Neurol. 1993; 33:4–9.
Article5. de Groot K, Schmidt DK, Arlt AC, Gross WL, Reinhold-Keller E. Standardized neurologic evaluations of 128 patients with Wegener granulomatosis. Arch Neurol. 2001; 58:1215–21.
Article6. Schedel J, Kuchenbuch S, Schoelmerich J, Feuerbach S, Geissler A, Mueller-Ladner U. Cerebral lesions in patients with connective tissue diseases and systemic vasculitides: are there specific patterns? Ann N Y Acad Sci. 2010; 1193; 167–75.
Article7. Provenzale JM, Allen NB. Wegener granulomatosis: CT and MR findings. AJNR Am J Neuroradiol. 1996; 17:785–92.8. Fuchs M, Briel M, Daikeler T, Walker UA, Rasch H, Berg S, et al. The impact of 18F-FDG PET on the management of patients with suspected large vessel vasculitis. Eur J Nucl Med Mol Imaging. 2012; 39:344–53.
Article9. Ueda N, Inoue Y, Himeji D, Shimao Y, Oryoji K, Mitoma H, et al. Wegener's granulomatosis detected initially by in-tegrated 18F-fluorodeoxyglucose positron emission tomography/computed tomography. Mod Rheumatol. 2010; 20:205–9.
Article10. Almuhaideb A, Syed R, Iordanidou L, Saad Z, Bomanji J. Fluorine-18-fluorodeoxyglucose PET/CT rare finding of a unique multiorgan involvement of Wegener's granulomatosis. Br J Radiol. 2011; 84:e202–4.
Article11. Beggs AD, Hain SF. F-18 FDG-positron emission tomo-graphic scanning and Wegener's granulomatosis. Clin Nucl Med. 2002; 27:705–6.
Article12. Seo P, Min YI, Holbrook JT, Hoffman GS, Merkel PA, Spiera R, et al. WGET Research Group. Damage caused by Wegener's granulomatosis and its treatment: prospective data from the Wegener's Granulomatosis Etanercept Trial (WGET). Arthritis Rheum. 2005; 52:2168–78.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Cortical Vein Thrombosis in Wegener's Granulomatosis
- A Case of Wegener's Granulomatosis Presenting with Cerebral Infarction and Intracerebral Hemorrhage
- Facial Palsy as a Presenting Symptom of Wegener's Granulomatosis
- A Case of Wegener's Granulomatosis Mimicking Behcet's Disease
- Localized Wegener's Granulomatosis in Maxillary Sinus
