Ann Dermatol.
2009 May;21(2):150-153. 10.5021/ad.2009.21.2.150.
A Case of Inflammatory Disseminated Superficial Porokeratosis in a Colon Cancer Patient
- Affiliations
-
- 1Department of Dermatology, College of Medicine, The Catholic University of Korea, Seoul, Korea. tykimderma@ catholic.ac.kr
- KMID: 2219384
- DOI: http://doi.org/10.5021/ad.2009.21.2.150
Abstract
- Disseminated superficial porokeratosis (DSP) is a specific disorder of keratinization. Genetic studies show that DSP is an autosomal dominant trait. Clinically, the lesions show a sharply demarcated and hyperkeratotic plaque with central atrophy. The lesions appear mainly in the extremities and generally develop with bilateral symmetry. Unusual cases of DSP accompanied by severe pruritus have been reported as "eruptive pruritic papular porokeratosis" or "inflammatory DSP." Histopathologically, inflammatory DSP is characterized by the presence of cornoid lamella with a dense infiltration of eosinophils and lymphocytes in the perivascular area of the upper dermis. Here we report a case of inflammatory DSP in a 84-year-old man with colon cancer who presented with multiple hyperpigmented atrophic macules.
MeSH Terms
Figure
-

Fig. 1 Disseminated brown annular plaques with hyperkeratotic borders on the trunk and extremities.
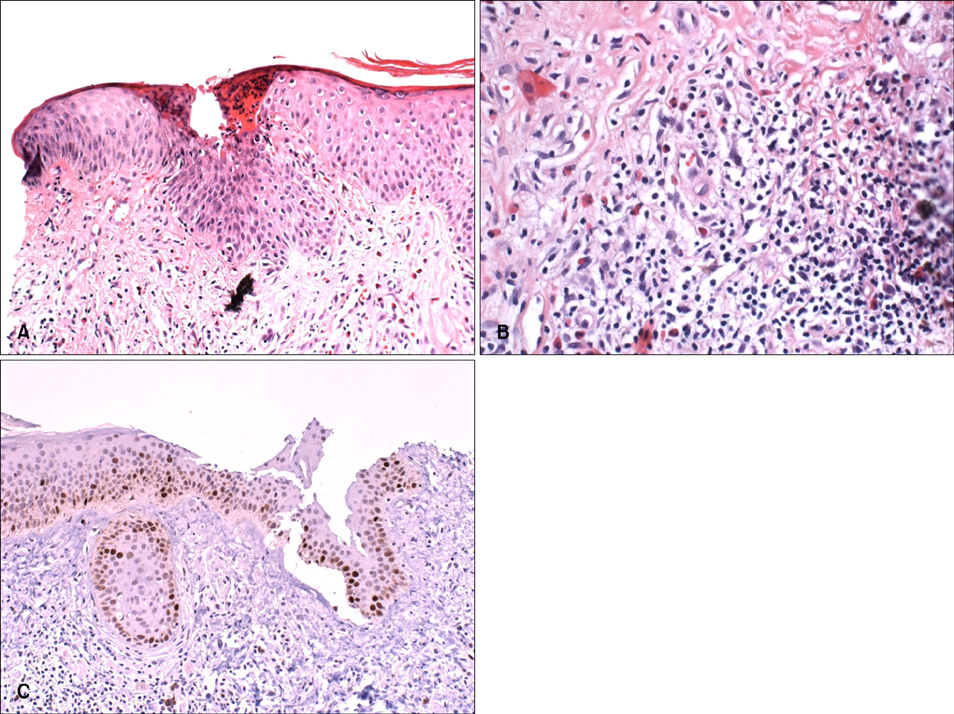
Fig. 2 (A) Histopathology of porokeratosis from the abdomen showing cornoid lamella; a column of parakeratotic cells (H&E stain, ×100). (B) Histopathology showing infiltrates with lymphocytes and eosinophils in the upper dermis and deeper dermis (H&E stain, ×200). (C) p53 staining showing strong nuclear reactivity on the basal layer of the lesion (labeled streptavidin-biotin-peroxidase complex) (×200).
Reference
-
1. O'Regan GM, Irvine AD. Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, editors. Prokeratosis. Fitzpatrick's dermatology in general medicine. 2008. 7th ed. New York: McGraw-Hill;568–574.2. Kanzaki T, Miwa N, Kobayashi T, Ogawa S. Eruptive pruritic papular porokeratosis. J Dermatol. 1992. 19:109–112.
Article3. Tanaka M, Terui T, Kudo K, Tagami H. Inflammatory disseminated superficial porokeratosis followed by regression. Br J Dermatol. 1995. 132:153–155.
Article4. Makino E, Inaoki M, Fujimoto W. Inflammatory stage of disseminated superficial porokeratosis. J Dermatol. 2005. 32:890–893.
Article5. Kanekura T, Yoshii N. Eruptive pruritic papular porokeratosis: a pruritic variant of porokeratosis. J Dermatol. 2006. 33:813–816.
Article6. Reed RJ, Leone P. Porokeratosis--a mutant clonal keratosis of the epidermis. I. Histogenesis. Arch Dermatol. 1970. 101:340–347.
Article7. Wei S, Yang S, Lin D, Li M, Zhang X, Bu L, et al. A novel locus for disseminated superficial porokeratosis maps to chromosome 18p11.3. J Invest Dermatol. 2004. 123:872–875.
Article8. Magee JW, McCalmont TH, LeBoit PE. Overexpression of p53 tumor suppressor protein in porokeratosis. Arch Dermatol. 1994. 130:187–190.
Article9. Takata M, Shirasaki F, Nakatani T, Takehara K. Hereditary non-polyposis colorectal cancer associated with disseminated superficial porokeratosis. Microsatellite instability in skin tumours. Br J Dermatol. 2000. 143:851–855.
Article10. Kono T, Kobayashi H, Ishii M, Nishiguchi S, Taniguchi S. Synchronous development of disseminated superficial porokeratosis and hepatitis C virus-related hepatocellular carcinoma. J Am Acad Dermatol. 2000. 43:966–968.
Article11. Lee HW, Oh SH, Choi JC, Chang SE, Lee MW, Choi JH, et al. Disseminated superficial porokeratosis in a patient with cholangiocarcinoma. J Am Acad Dermatol. 2006. 54:S56–S58.
Article12. McDonald SG, Peterka ES. Porokeratosis (Mibelli): treatment with topical 5-fluorouracil. J Am Acad Dermatol. 1983. 8:107–110.
Article13. Dereli T, Ozyurt S, Ozturk G. Porokeratosis of Mibelli: successful treatment with cryosurgery. J Dermatol. 2004. 31:223–227.
Article14. Barnett JH. Linear porokeratosis: treatment with the carbon dioxide laser. J Am Acad Dermatol. 1986. 14:902–904.
Article15. Liu HT. Treatment of lichen amyloidosis (LA) and disseminated superficial porokeratosis (DSP) with frequency-doubled Q-switched Nd:YAG laser. Dermatol Surg. 2000. 26:958–962.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Exacerbation of Disseminated Superficial Actinic Porokeratosis in a Patient with Colon Cancer
- Inflammatory Disseminated Superficial Porokeratosis Successfully Managed by Oral Isotretinoin
- Coexistence of Porokeratosis of Mibelli and Disseminated Superficial Actinic Porokeratosis
- Inflammatory Disseminated Superficial Porokeratosis
- A Case of Linear Porokeratosis Superimposed on Disseminated Superficial Actinic Porokeratosis
