Two Cases of Corneal Toxicity in Acanthamoeba Keratitis by Combined Topical Anti-Acanthamoeba Keratitis Eye Solution
- Affiliations
-
- 1Department of Ophthalmology, Pusan National University School of Medicine, Busan, Korea. jongsool@pusan.ac.kr
- 2Biomedical Research Institute, Pusan National University Hospital, Busan, Korea.
- KMID: 2216014
- DOI: http://doi.org/10.3341/jkos.2015.56.2.280
Abstract
- PURPOSE
To present a case of corneal toxicity caused by therapeutic duplication during treatment of acanthamoeba keratitis as a complication of contact lens use.
CASE SUMMARY
A 12-year-old girl with a history of wearing orthokeratology contact lenses and a 14-year-old girl with a history of wearing cosmetic contact lenses presented with ocular pain, injection, and decreased visual acuity. They were diagnosed as having acanthamoeba keratitis based on slit lamp examination, confocal microscopy and culture. After the patients were treated with polyhexamethylene biguanide (PHMB) and chlorhexidine, corneal epithelial defect and erosion occurred. Use of chlorhexidine was stopped, and PHMB was used to treat patients and recovery of the corneal epithelium with improvement in symptoms of acanthamoeba keratitis was found.
CONCLUSIONS
Using PHMB and chlorhexidine together in treating acanthamoeba keratitis increases the risk of corneal toxicity. Therefore, these drugs should be avoided in combination.
MeSH Terms
Figure
-
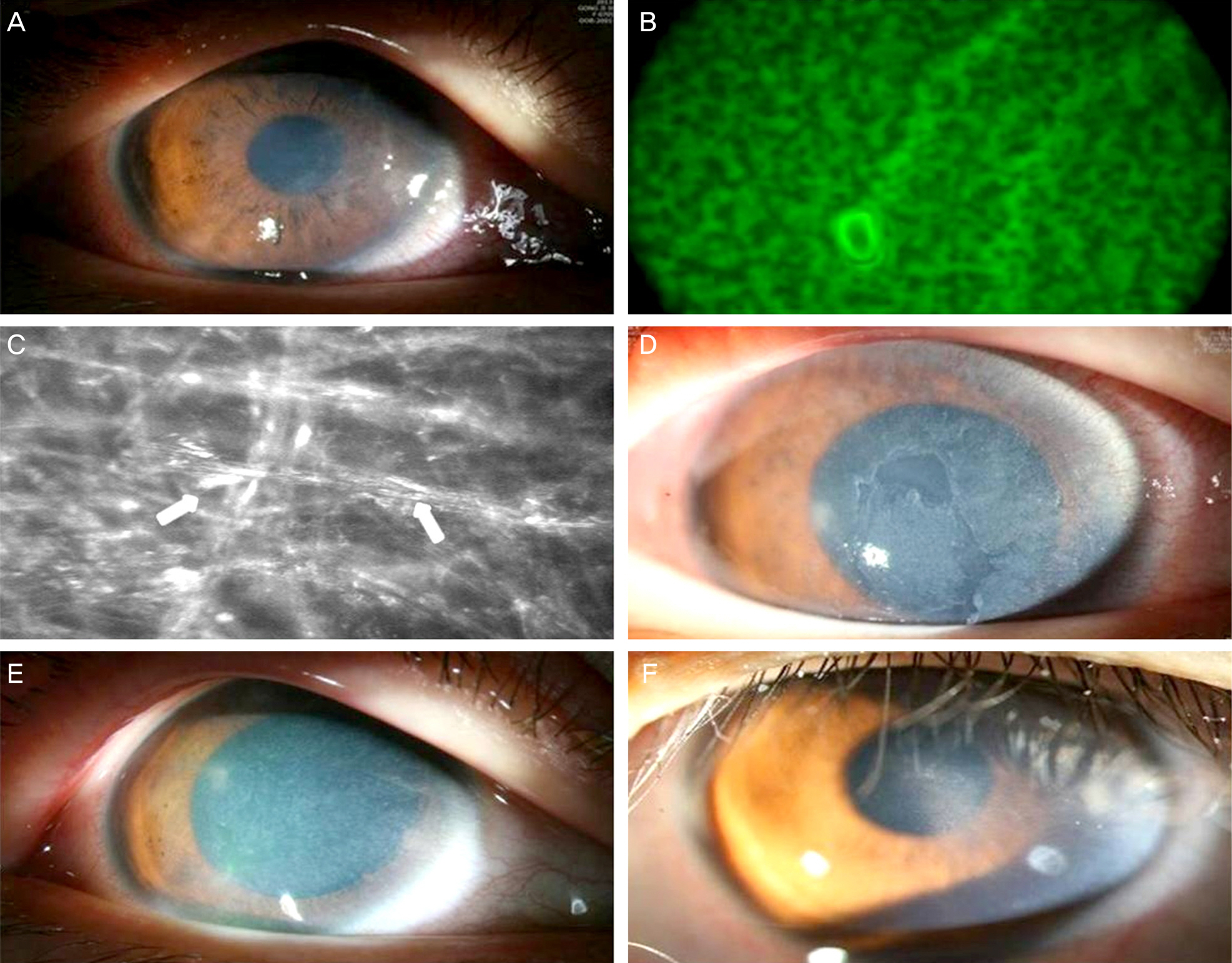
Figure 1. (A) Slit-lamp photograph and flurescein stain of the right cornea of a 12-years-old girl with a history of wearing orthoker-atology contact lenses. (B) Acanthamoeba track on the culture on E. coli plated agar media from contact lens. (C) In vivo laser confocal microscopic images of the right cornea. In the stroma numerous highly reflective, spindle-shaped materials were aggravated (arrows). (D) Slit-lamp photograph and ulcerated lesion was stained under PHMB and chlorhexidine administration. (E) After 1 day of stopping chlorhexidine use, corneal and conjunctival lesion improved. (F) After 2 months, residual corneal subepithelial opacity remained, and no corneal stain lesion is seen. PHMB = polyhexamethylene biguanide.
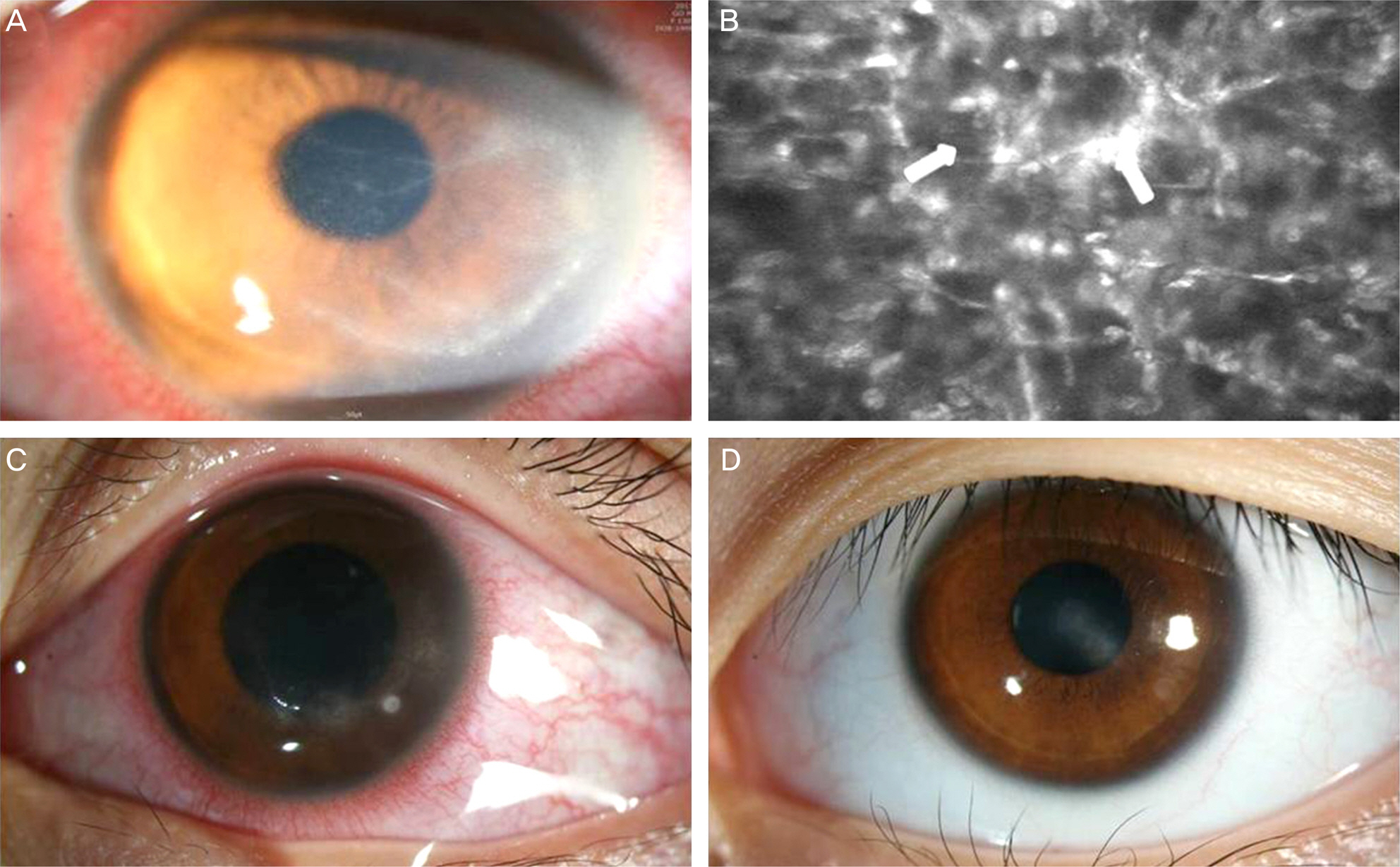
Figure 2. (A) A 14-year-old girl with a history of wearing cosmetic contact lenses presented with corneal circinate infiltrate in the left eye. (B) In vivo laser confocal microscopic images of the cornea of the left eye of case 2. In the stroma around the keratoneuritis, highly reflective activated keratocytes formed a honeycomb pattern (arrows). (C) Punctate epithelial keratitis, corneal haze, con-junctival injection, and perilimbal vascularization are observed under PHMB and chlorhexidine administration. (D) After 5 months; residual mild corneal opacity remains. PHMB = polyhexamethylene biguanide.
Reference
-
References
1. Naginton J, Watson PG, Playfair TJ. . Amoebic infection of the eye. Lancet. 1974; 2:1537–40.2. Wilhelmus KR. Introduction: the increasing importance of Acanthamoeba. Rev Infect Dis. 1991; 13(Suppl 5):S367–8.
Article3. Steinemann TL, Fletcher M, Bonny AE. . Over-the-counter decorative contact lenses: Cosmetic or Medical Devices? A Case Series. Eye Contact Lens. 2005; 31:194–200.
Article4. Cohen EJ, Parlato CJ, Arentsen JJ. . Medical and surgical treatment of Acanthamoeba keratitis. Am J Ophthalmol. 1987; 103:615–25.
Article5. Bacon AS, Frazer DG, Dart JK. . A review of 72 consecutive cases of Acanthamoeba keratitis, 1984-1992. Eye (Lond). 1993; 7(Pt 6):719–25.
Article6. Moore MB, McCulley JP, Luckenbach M. . Acanthamoeba keratitis associated with soft contact lenses. Am J Ophthalmol. 1985; 100:396–403.
Article7. Larkin DF, Kilvington S, Dart JK. Treatment of Acanthamoeba keratitis with polyhexamethylene biguanide. Ophthalmology. 1992; 99:185–91.
Article8. Hay J, Kirkness CM, Seal DV, Wright P. Drug resistance and Acanthamoeba keratitis: the quest for alternative antiprotozoal chemotherapy. Eye (Lond). 1994; 8(Pt 5):555–63.
Article9. Seal DV, Hay J, Kirkness CM. Chlorhexidine or polyhexamethylene biguanide for acanthamoeba keratitis. Lancet. 1995; 345:136.
Article10. Lee JE, Oum BS, Choi HY. . Cysticidal effect on acanthamoeba and toxicity on human keratocytes by polyhexamethylene biguanide and chlorhexidine. Cornea. 2007; 26:736–41.
Article11. Green K, Livingston V, Bowman K, Hull DS. Chlorhexidine effects on corneal epithelium and endothelium. Arch Ophthalmol. 1980; 98:1273–8.
Article12. Goldschmidt P, Cogen R, Taubman S. Cytopathologic effects of chlorhexidine on human cells. J Periodontol. 1977; 48:212–5.
Article13. Murthy S, Hawksworth NR, Cree I. Progressive ulcerative keratitis related to the use of topical chlorhexidine gluconate (0.02%). Cornea. 2002; 21:237–9.
Article14. Smolin G, Thoft RA. The Cornea: Scientific Foundations and Clinical Practice. 3rd ed.Little, Brown & Company;1994. p. 88–9.15. Seal D, Hay J, Kirkness C. . Successful medical therapy of Acanthamoeba keratitis with topical chlorhexidine and propamidine. Eye (Lond). 1996; 10(Pt 4):413–21.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acanthoamoeba Keratitis Induced by a Therapeutic, Soft Contact Lens: Diagnosis via Gram Staining
- Acanthamoeba Keratitis Related to Orthokeratology Contact Lens
- In vivo tandem scanning confocal microscopy in acanthamoeba keratitis
- Comparison of Usefulness of Laboratory Diagnosis in Ancanthamoeba Keratitis
- Molecular detection and characterization of Acanthamoeba infection in dogs and its association with keratitis in Korea
