J Korean Ophthalmol Soc.
2012 Jan;53(1):157-160. 10.3341/jkos.2012.53.1.157.
A Case of Iatrogenic Horner's Syndrome after Video-Thoracoscopic Surgery for Primary Pneumothorax
- Affiliations
-
- 1Department of Ophthalmology, Busan Paik Hospital, Inje University College of Medicine, Busan, Korea. eyeyang@inje.ac.kr
- 2Department of Thoracic and Cardiovascular Surgery, Busan Paik Hospital, Inje University College of Medicine, Busan, Korea.
- KMID: 2215259
- DOI: http://doi.org/10.3341/jkos.2012.53.1.157
Abstract
- PURPOSE
To report a case of iatrogenic Horner's syndrome after video-thoracoscopic surgery for primary pneumothorax.
CASE SUMMARY
An 18-year-old man with ptosis in the right eye was referred to our clinic. The patient had undergone wedge resection via video-thoracoscopic surgery for primary pneumothorax three weeks previously. On ocular examination, the palpebral fissure width was 7 mm in the right lid and 8 mm in the left lid, the marginal reflex distance 1 (MRD 1) was 2 mm in the right lid and 3 mm in the left lid, and the bilateral levator muscle function was good. Anisocoria was present, and pupil size in a dark room was 2.5 mm in the right eye and 4 mm in the left eye. The patient complained of facial anhidrosis on the right side of the face.
CONCLUSIONS
Although iatrogenic Horner's syndrome is rare complication of video-thoracoscopic surgery for primary pneumothorax, diagnosis after surgery of the thoracic cavity should be made carefully.
MeSH Terms
Figure
-
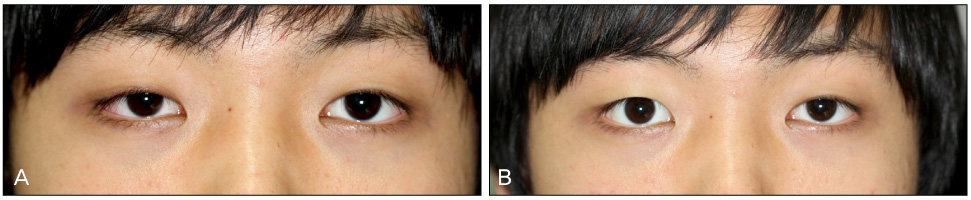
Figure 1 Photographs of an 18-year-old man who underwent chest tube insertion into the right thoracic cavity. (A) Photograph showing 1 mm of right upper eyelid ptosis and anisocoria. (B) Right upper eyelid ptosis and miosis improved after instilling 1% phenylephrine.

Figure 2 Chest X-ray showing that tip of chest tube is positioned at T5 level in thoracic caivity. The multiple clips and resection lines for apical lung bullectomy are noted on both sided upper lobes.

Figure 3 Photograph of 1 week after mullerectomy. Ptosis is improved by mullerectomy 4 months after the symptom developed.
Reference
-
1. Walton KA, Buono LM. Horner syndrome. Curr Opin Ophthalmol. 2003. 14:357–363.2. Gallagher PG, Benzing G 3rd. Iatrogenic Horner's syndrome. J Crit Care. 1990. 5:238–240.3. Kaya SO, Liman ST, Bir LS, et al. Horner's syndrome as a complication in thoracic surgical practice. Eur J Cardiothorac Surg. 2003. 24:1025–1028.4. Sataline LR, Kraus T. Horner's syndrome occurring with spontaneous pneumothorax. N Engl J Med. 1965. 272:1227–1228.5. Aston SJ, Rosove M. Horner's syndrome occurring with spontaneous pneumothorax. N Engl J Med. 1972. 287:1098.6. Cook T, Kietzman L, Leibold R. "Pneumo-ptosis" in the emergency department. Am J Emerg Med. 1992. 10:431–434.7. Osterman PO, Osterman K. Reversible Horner's syndrome associated with spontaneous pneumothorax. Scand J Respir Dis. 1971. 52:230–231.8. Thakar C, Hunt I, Anikin V. Horner's syndrome in a patient presenting with a spontaneous pneumothorax. Emerg Med J. 2008. 25:119–120.9. Zagrodnik DF 2nd, Kline AL. Horner's syndrome: a delayed complication after thoracostomy tube removal. Curr Surg. 2002. 59:96–98.10. Jo YJ, Lee YH, Yun YJ, Lee SB. Iatrogenic Horner's syndrome after procedure in the neck and upper thoracic area. J Korean Ophthalmol Soc. 2009. 50:809–815.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Horner's Syndrome: A Rare Complication of Tube Thoracostomy: A case report
- Video-assisted Thoracioscopic Surgery under Epidural Anesthesia in the High-Risk Patients with Secondary Spontaneous Pneumothorax
- Thoracoscopic Bleb Ligation in Patients with Primary Spontaneous Pneumothorax
- Bullectomy Using 2 mm Videothoracoscope in Primary Spontaneous Pneumothorax
- Comparision of Clinical Results of Video-Assisted Thoracoscopic Surgery and Axillary Mini-Thoractomy for Spontaneous Pneumothorax
