Spontaneous Eyeball Rupture in a 94-Year-Old Patient
- Affiliations
-
- 1Department of Ophthalmology, Bundang CHA Hospital, CHA University, Seongnam, Korea. eye@cha.ac.kr
- 2Department of Pathology, Bundang CHA Hospital, CHA University, Seongnam, Korea.
- KMID: 2214647
- DOI: http://doi.org/10.3341/jkos.2011.52.6.734
Abstract
- PURPOSE
To report a case of spontaneous eye ball rupture without trauma in a 94-year-old patient.
CASE SUMMARY
A 94-year-old female patient diagnosed with cataract in both eyes 20 years was referred to this ophthalmologic department for treatment consultation of a painful left eye with spontaneous bleeding. She has used anti-cataract eye drops and artificial tears three times a day for several years without consulting a doctor. Fifteen days prior to presentation, the patient suffered severe left eyeball pain and headache and was diagnosed with acute angle-closure glaucoma secondary to hypermature cataract. She underwnet eviceration after ocular examination and systemic evaluation. Surgical findings included a thin cornea at the inferior limbus and protruding intraocular tissues. Additionally, the eyeball was filled with a blood clot from a choroidal hemorrhage. Morganella morganii were grown in a bacterial swap culture, and a corneal biopsy revealed suppurative inflammation.
CONCLUSIONS
In old age, a thin corneal limbus due to infection and complicated acute angle-closure glaucoma can cause massive suprachoroidal hemorrhage with spontaneous eyeball rupture.
Keyword
MeSH Terms
Figure
-

Figure 1. (A) Ruptured left eye ball with protruded intraocular tissues and conjunctival hemorrhage are noted in the 94-year-old female patient. (B) Axial image of orbital CT shows irregular anterior margin of the left eye ball filled with hemorrhage.
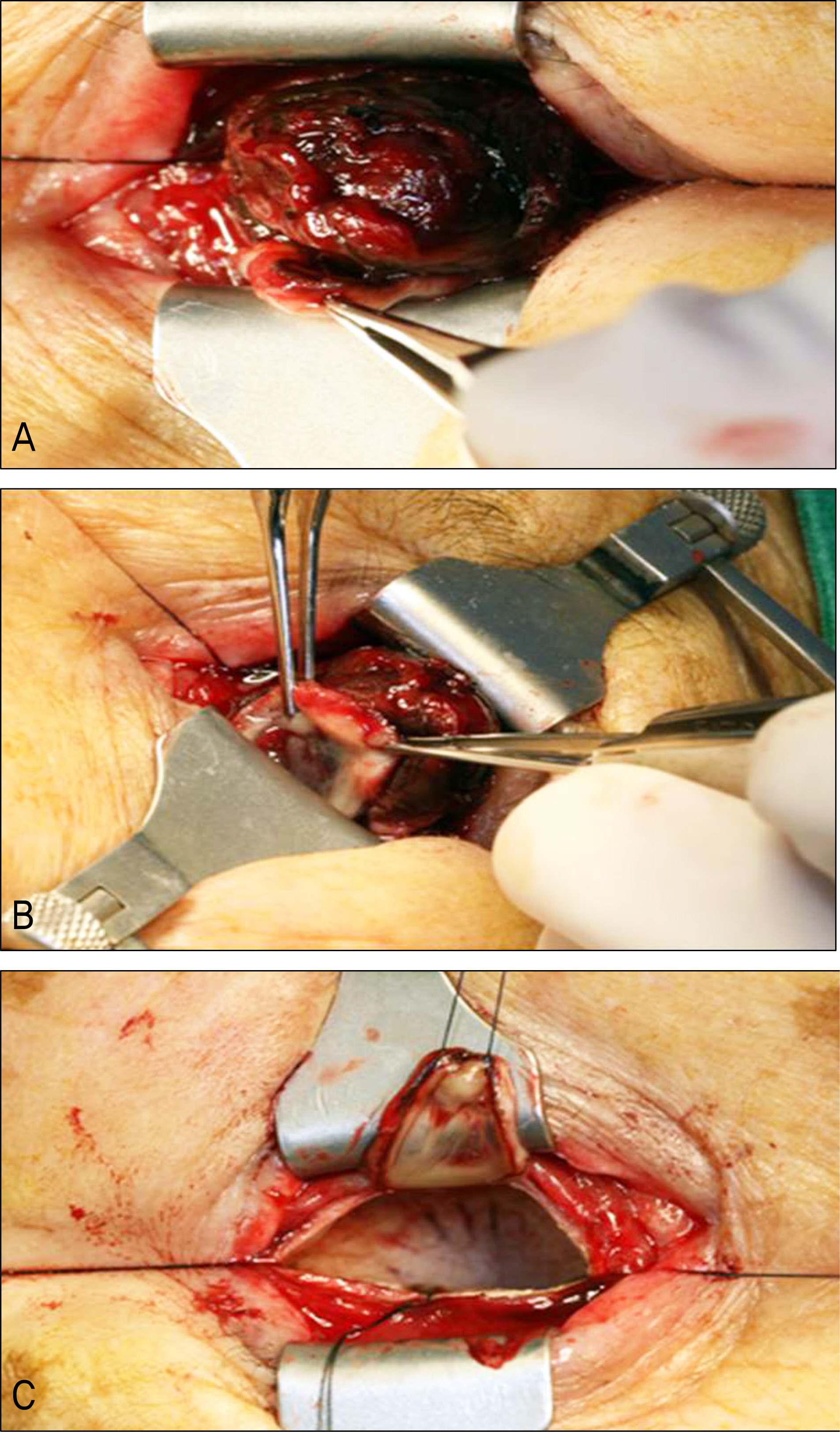
Figure 2. Intraoperative findings. (A) Protruding intraocular tissues are noted. (B) The cornea is very thin and perforated along the inferior corneoscleral junction. (C) After removal of intra ocular tissues, the posterior part is intact.
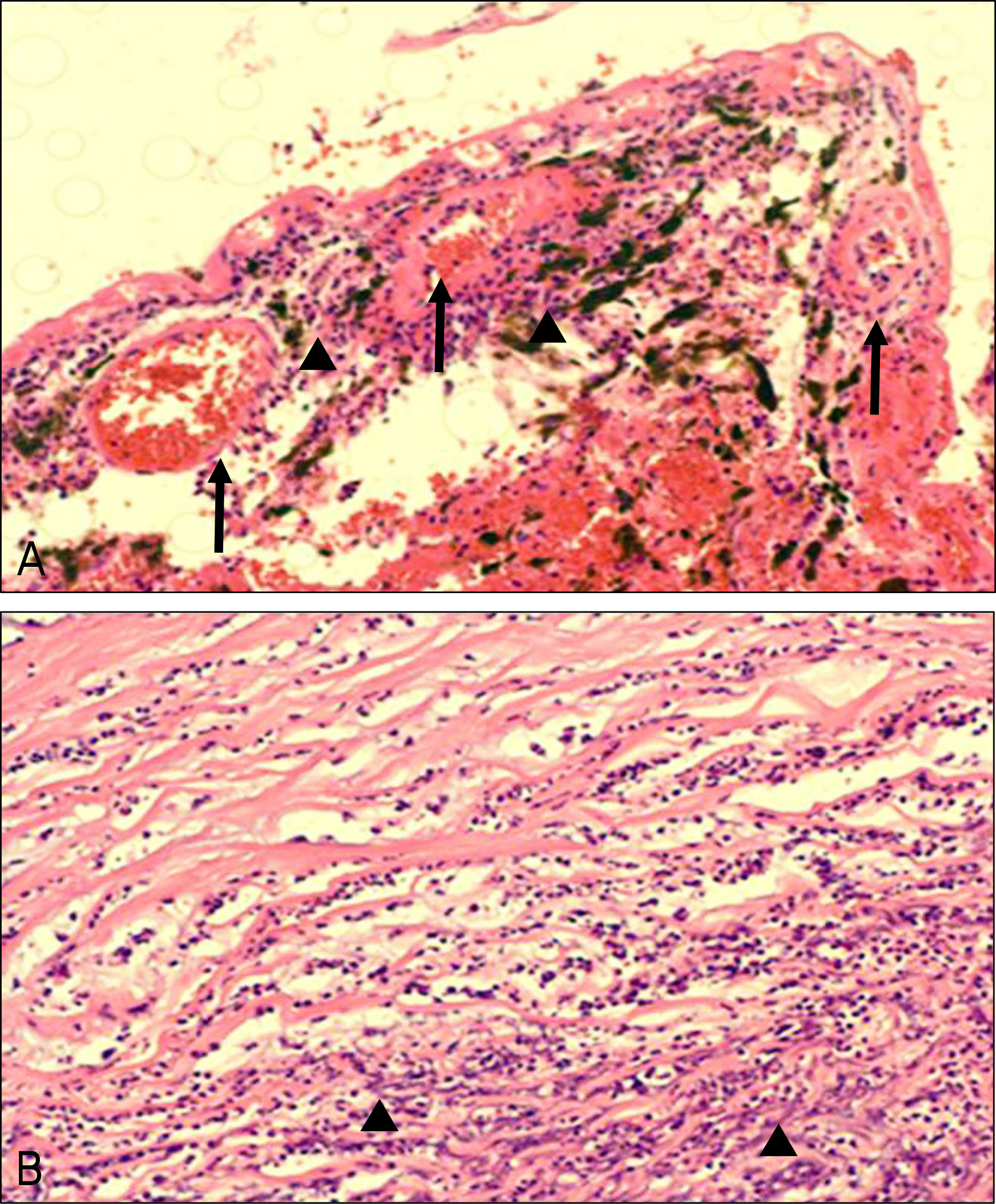
Figure 3. (A) Choroidal vessels (arrow) with blood clots, inflammatory cells (arrowhead) surrounding vessel wall are noted (H&E stain, ×200). (B) Corneal biopsy specimen presents diffuse supprative inflammation in the stroma. Stromal infiltrations of many lymphocytes are noted (arrowhead) (H&E stain, ×200).
Reference
-
References
1. Rutherford WJ. Spontaneous rupture of the glaucomatous eye: an illustrative case. Br J Ophthalmol. 1920; 4:282–4.
Article2. Winslow RL, Stevenson W 3rd, Yanoff M. Spontaneous expulsive choroidal hemorrhage. Arch Ophthalmol. 1974; 92:33–6.
Article3. Goldsmith C, Rene C. Massive spontaneous expulsive suprachoroidal haemorrhage in a blind glaucomatous eye treated with chronic topical steroid. Eye (Lond). 2003; 17:439–40.
Article4. Ophir A, Pikkel J, Groisman G. Spontaneous expulsive suprachoroidal hemorrhage. Cornea. 2001; 20:893–6.
Article5. Haugen OH, Kjeka O. Localized, extreme scleral thinning causing globe rupture during strabismus surgery. J AAPOS. 2005; 9:595–6.
Article6. Ung T, Williams CP, Canning CR. Globe rupture as a complication of intravitreal injection of triamcinolone. Eye (Lond). 2007; 21:423–4.
Article7. Tabandeh H, Flaxel C, Sullivan PM, et al. Scleral rupture during retinal detachment surgery: risk factors, management options, and outcomes. Ophthalmology. 2000; 107:848–52.8. Awad AH, Mullaney PB, Al-Hazmi A, et al. Recognized globe perforation during strabismus surgery: incidence, risk factors, and sequelae. J AAPOS. 2000; 4:150–3.
Article9. Dang Y, Racu C, Isenberg SJ. Scleral penetrations and perforations in strabismus surgery and associated risk factors. J AAPOS. 2004; 8:325–31.
Article10. Warwick R. Eugene Wolff's Anatomy of the Eye and Orbit. 7th ed.London: HK Lewis & Co;1976. p. 48–51.11. Fleming A, Dodman S, Crown JM, Corbett M. Extra-articular features in early rheumatoid disease. Br Med J. 1976; 1:1241–3.
Article12. Sipperley JO, Shore JW. Septic retinal cyst in endogenous Klebsiella endophthalmitis. Am J Ophthalmol. 1982; 94:124–5.
Article13. Tae KS, Kim TH, Moon YS, Chin HS. A case of klebsiella endogenous endophthalmitis accompanied by necrotizing scleral perforation. J Korean Ophthalmol Soc. 2003; 11:2680–6.14. Equi RA, Green WR. Endogenous Serratia marcescens endophthalmitis with dark hypopyon: case report and review. Surv Ophthalmol. 2001; 46:259–68.15. Taherian K, Sharma P, Prakash P, Azad R. Scleral perforations in strabismus surgery: incidence and role of prophylactic cryotherapy–a clinical and experimental study. Strabismus. 2004; 12:17–25.16. Yu YS, Chang BL. Scleral perforation after scleral buckling surgery for retinopathy of prematurity. Korean J Ophthalmol. 1999; 13:49–51.
Article17. Kwon JD, Kim SW, Park DH, Lee CH. A case of a traumatic eye-ball rupture in terrien's marginal degeneration and it's surgical repair. J Korean Ophthalmol Soc. 2006; 47:1166–70.18. Cunningham ET Jr, Whitcher JP, Kim RY. Morganella morganii postoperative endophthalmitis. Br J Ophthalmol. 1997; 81:170–1.
Article19. Tsanaktsidis G, Agarwal SA, Maloof AJ, et al. Postoperative Morganella morganii endophthalmitis associated with subclinical urinary tract infection. J Cataract Refract Surg. 2003; 29:1011–3.
Article20. Burstein NL. Preservative cytotoxic threshold for benzalkonium chloride and chlorhexidine digluconate in cat and rabbit corneas. Invest Ophthalmol Vis Sci. 1980; 19:308–13.22. Tripathi BJ, Tripathi RC. Cytotoxic effects of benzalkonium chloride and chlorobutanol on human corneal epithelial cells in vitro. Lens Eye Toxic Res. 1989; 6:395–403.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Spontaneous Splenic Rupture
- A Case of Spontaneous Rupture of Renal Pelvis without Identifiable Cause Treated Conservatively
- A Case of Spontaneous Rupture of the Kidney
- Spontaneous rupture of the esophagus associated with intramural rupture caused by ingestion of weedi...
- Two Cases of Spontaneous Rupture of the Kidney
