J Korean Surg Soc.
2013 Aug;85(2):93-95. 10.4174/jkss.2013.85.2.93.
Open surgical decompression of celiac axis compression by division of the median arcuate ligament
- Affiliations
-
- 1Division of Vascular Surgery, Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. ywkim@skku.edu
- KMID: 2212524
- DOI: http://doi.org/10.4174/jkss.2013.85.2.93
Abstract
- Median arcuate ligament syndrome is a rare cause of abdominal pain which results from compression of the celiac artery (CA) or rarely, the superior mesenteric artery by a ligament formed by the right and left crura of the diaphragm. We report a case of open surgical decompression of the CA by division of the median arcuate ligament for a 37-year-old female patient who had suffered from chronic postprandial epigastric pain and severe weight loss. We described clinical features, characteristic angiographic findings and details of the surgical procedure for the patient with this rare vascular problem.
MeSH Terms
Figure
-
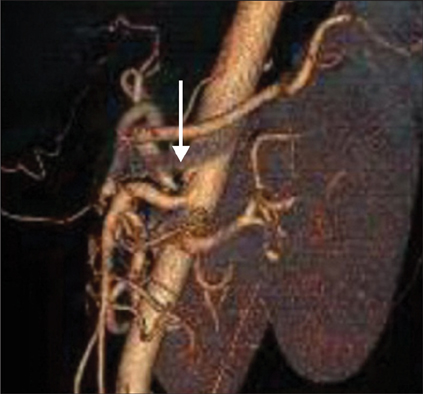
Fig. 1 Computed tomographic angiography: celiac trunk stenosis. Compression of celiac artery (CA) makes an acute angle of CA (arrow).
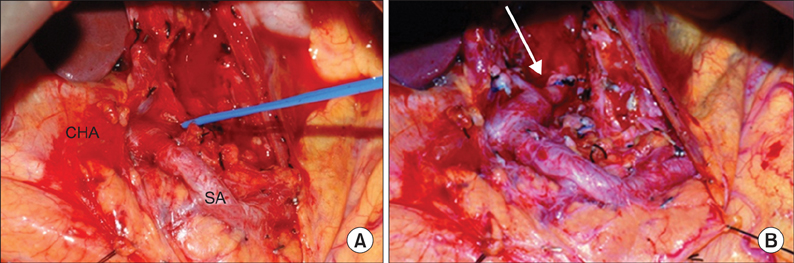
Fig. 2 Operative finding. (A) Fibrous structure (in a vessel loop) compressing celiac artery (CA). (B) Mild residual stenosis (arrow) of CA after division of fibrous structure. CHA, common hepatic artery; SA, splenic artery.

Fig. 3 Follow-up computed tomographic angiography. After surgical decompression of celiac artery (CA), downward angulation of CA disappeared (arrow).
Reference
-
1. Duffy AJ, Panait L, Eisenberg D, Bell RL, Roberts KE, Sumpio B. Management of median arcuate ligament syndrome: a new paradigm. Ann Vasc Surg. 2009. 23:778–784.2. Saddekni S, Sniderman KW, Hilton S, Sos TA. Percutaneous transluminal angioplasty of nonatherosclerotic lesions. AJR Am J Roentgenol. 1980. 135:975–982.3. Lipshutz B. A composite study of the coeliac axis artery. Ann Surg. 1917. 65:159–169.4. Harjola PT. A rare obstruction of the coeliac artery: report of a case. Ann Chir Gynaecol Fenn. 1963. 52:547–550.5. Dunbar JD, Molnar W, Beman FF, Marable SA. Compression of the celiac trunk and abdominal angina. Am J Roentgenol Radium Ther Nucl Med. 1965. 95:731–744.6. Skeik N, Cooper LT, Duncan AA, Jabr FI. Median arcuate ligament syndrome: a nonvascular, vascular diagnosis. Vasc Endovascular Surg. 2011. 45:433–437.7. Petrella S, Prates JC. Celiac trunk compression syndrome: a review. Int J Morphol. 2006. 24:429–436.8. Tulloch AW, Jimenez JC, Lawrence PF, Dutson EP, Moore WS, Rigberg DA, et al. Laparoscopic versus open celiac ganglionectomy in patients with median arcuate ligament syndrome. J Vasc Surg. 2010. 52:1283–1289.9. Gloviczki P, Duncan AA. Treatment of celiac artery compression syndrome: does it really exist? Perspect Vasc Surg Endovasc Ther. 2007. 19:259–263.10. Cinà CS, Safar H. Successful treatment of recurrent celiac axis compression syndrome: a case report. Panminerva Med. 2002. 44:69–72.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Laparoscopic management of median arcuate ligament syndrome: a video vignette
- Celiac Axis Compression Syndrome
- Celiac Axis Stenosis: Incidence and Etiologies in Asymptomatic Individuals
- Clinical and Radiologic Review of Uncommon Cause of Profound Iron Deficiency Anemia: Median Arcuate Ligament Syndrome
- Celiac axis stenosis as a rare but critical condition treated with pancreatoduodenectomy: report of 2 cases
