Clinical Outcomes of Toric Implantable Collamer Lens implantation
- Affiliations
-
- 1Department of Ophthalmology, Sungmo Eye Hospital, Busan, Korea. sungmo@sungmo.co.kr
- KMID: 2212360
- DOI: http://doi.org/10.3341/jkos.2009.50.6.839
Abstract
-
PURPOSE: To assess the efficacy of the Toric Implantable Collamer Lens (Toric ICL) to treat moderate to high myopic astigmatism.
METHODS
Toric ICL was implanted in 77 eyes of 40 patients with myopia (spherical equivalent [SE] between 3.5 and 18.5 diopters [D]) and astigmatism between 1 and 6 D. The patients were followed up for at least 3 months. Uncorrected visual acuity (UCVA), refraction, best spectacle-corrected visual acuity (BSCVA), adverse events, and postoperative complications were evaluated.
RESULTS
At 3months postoperatively, the proportion of eyes with 1.0 or better UCVA (56 eyes out of 77 eyes, 72.7%) was significantly greater than the proportion of eyes with preoperative 1.0 or better BSCVA (38 eyes out of 77 eyes, 49.4%). The mean manifest refractive cylinder dropped from 2.78D (+/-1.05) at baseline to 0.35D (+/-0.34) postoperatively, an 87.4% decrease in astigmatism. Mean manifest refraction SE (MRSE) improved from -9.93D (+/-2.66) preoperatively to 0.15D (+/-0.33) postoperatively. A total of 96.1% of eyes were predicted accurately to within +/-0.75D of predicted MRSE. Mean improvement in BSCVA was 0.79lines; there were no eyes that lost two lines of BSCVA after 3 months postoperatively.
CONCLUSIONS
The results support the efficacy and predictability of Toric ICL implantation to treat moderate to high myopic astigmatism.
Figure
-
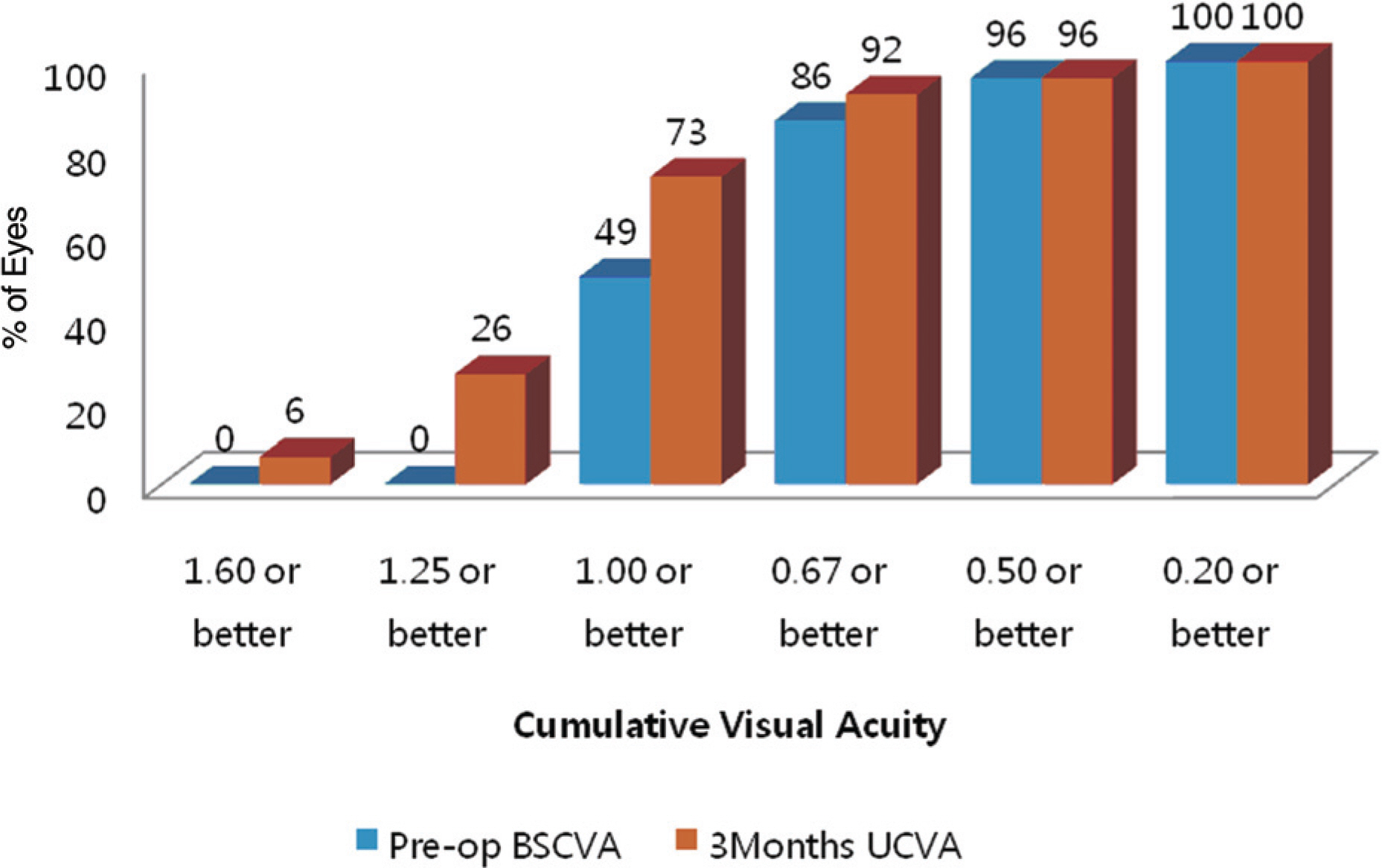
Figure 1. Preoperative (pre-op) best spectacle-corrected visual acuity (BSCVA) versus 3-month postoperative uncorrected visual acuity (UCVA) for the Toric Implantable Collamer Lens cohort.
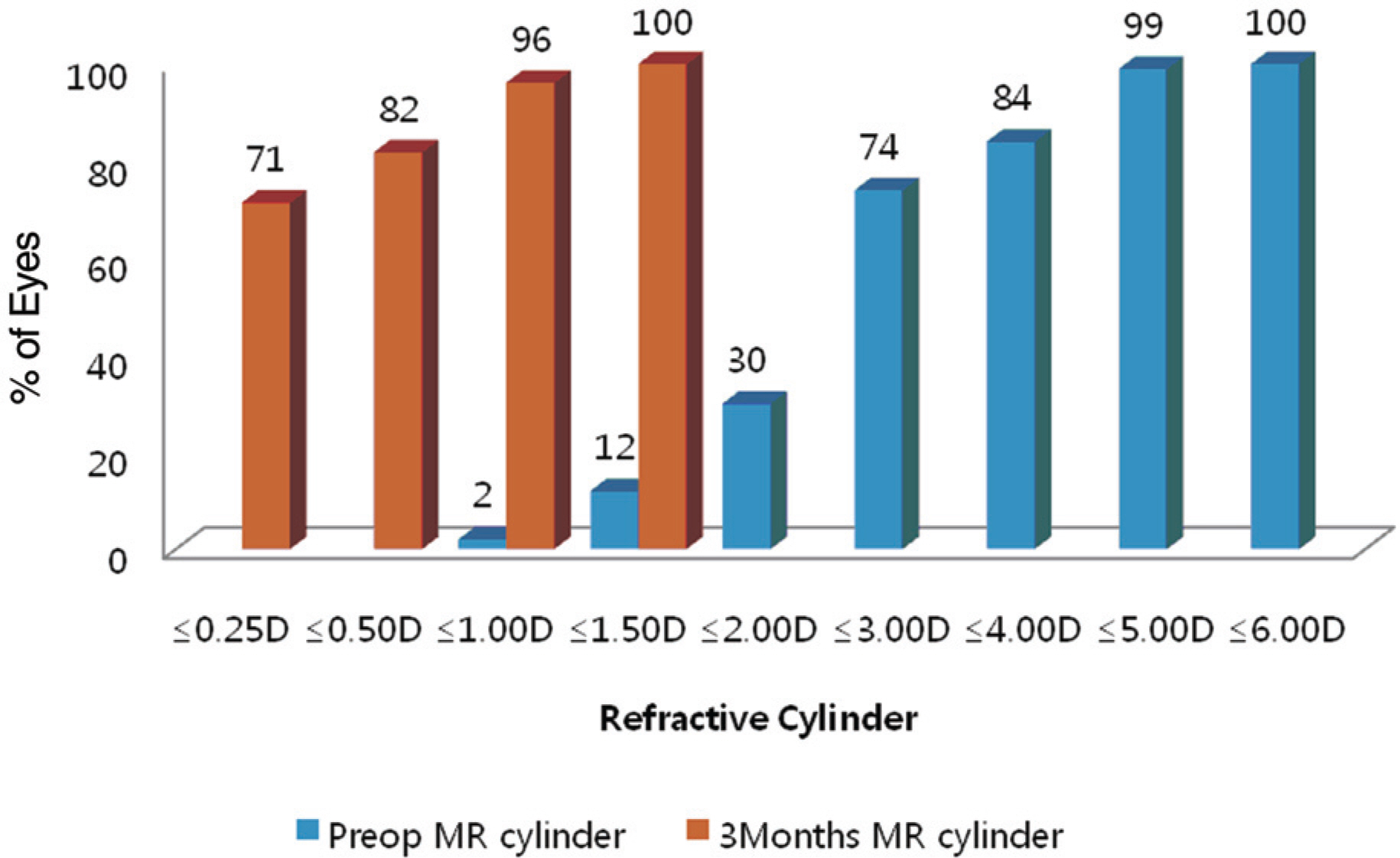
Figure 2. Preoperative (pre-op) versus 3-month post-operative refractive cylinder for the Toric Implantable Collamer Lens cohort (D=diopters; MR=manifest refraction).
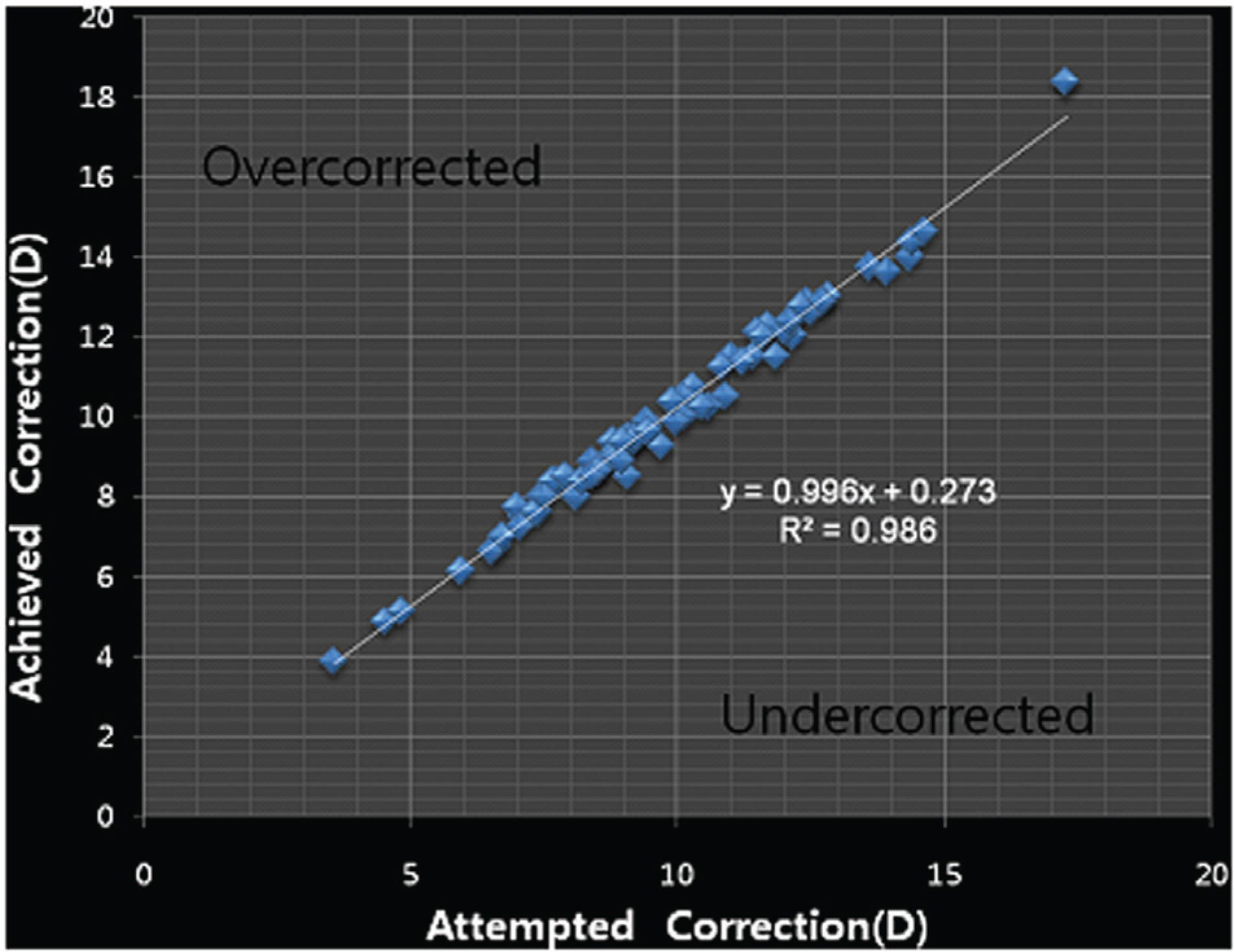
Figure 3. Attempted vs achieved spherical equivalent The difference between achieved spherical equivalent and attempted spherical equivalent is within 1diopter in most cases.
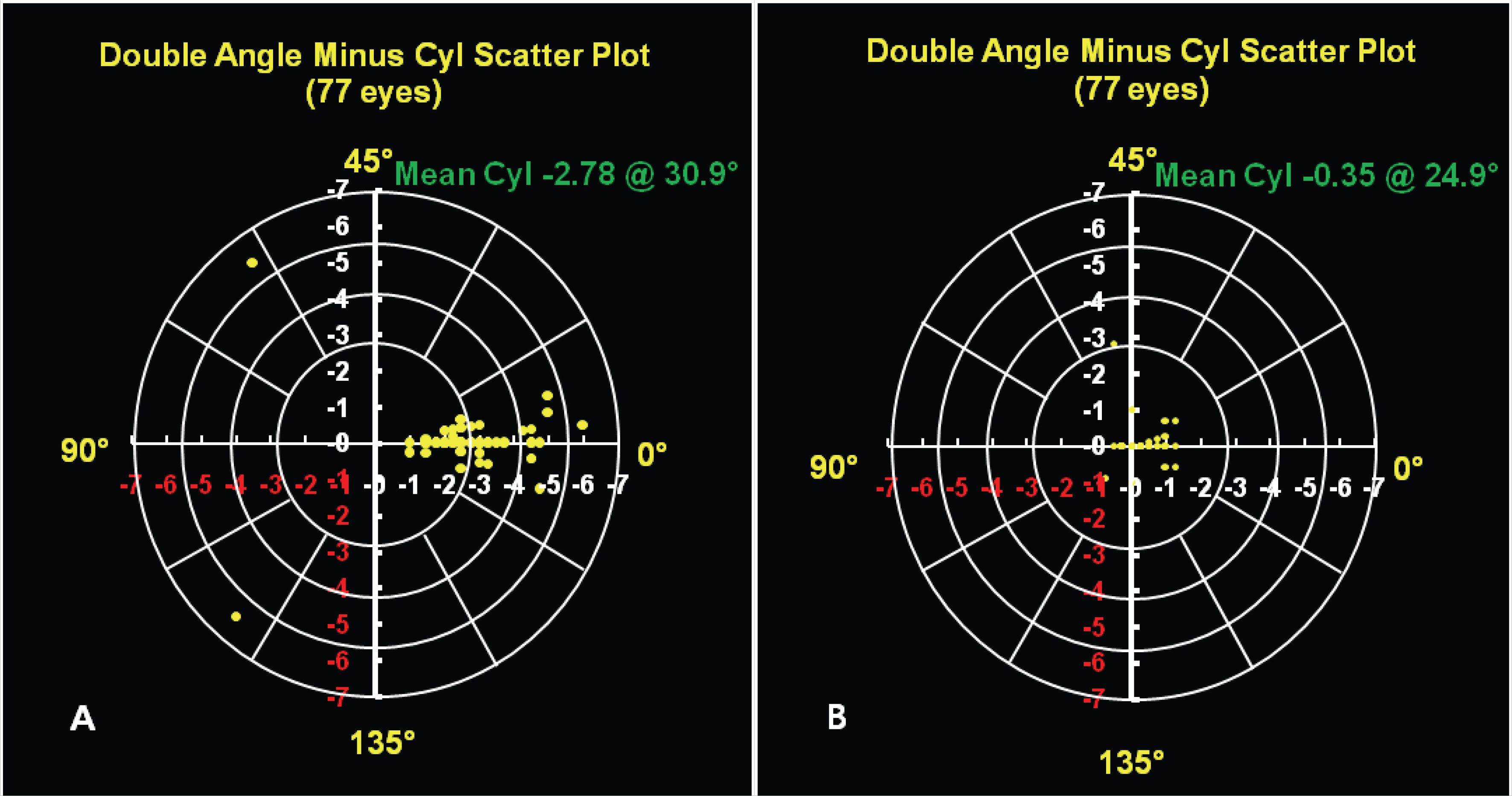
Figure 4. (A) Preoperative astigmatism. The yellow dots show preoperative astigmatism which consist of axis and diopter in the double angle scatter plot. It is scattered and the average of astigmatism is −2.75 diopter with 30.9° (B) 3-month postoperative astigmatism The yellow dots show postoperative astigmatism which consists of axis and diopter in the double angle scatter plot. It is not scattered but focused on zero point and the average of astigmatism is −0.35 diopter with 24.9°
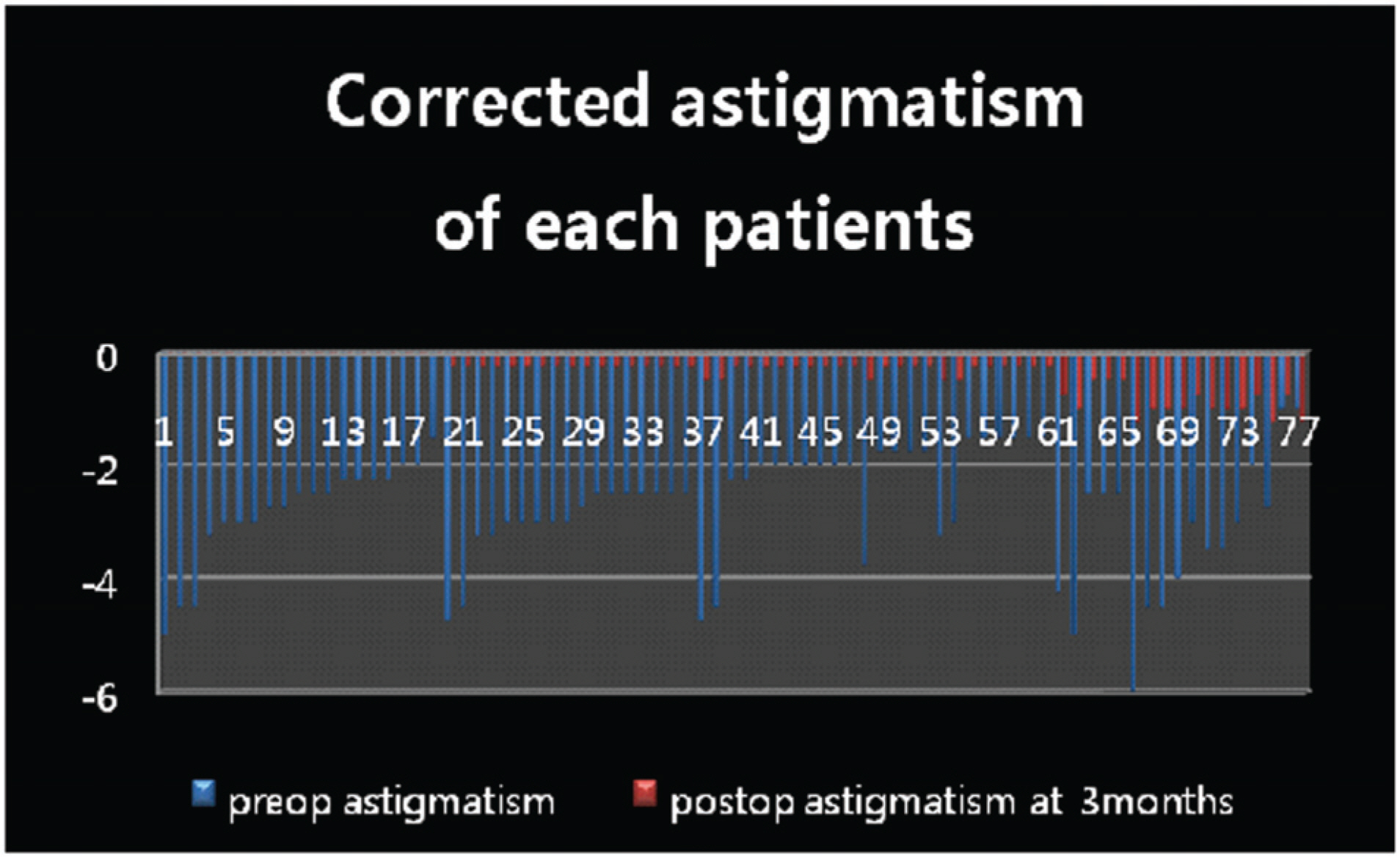
Figure 5. The amount of corrected astigmatism in each patient. In most of the patients, astigmatism decreased by about 86%.
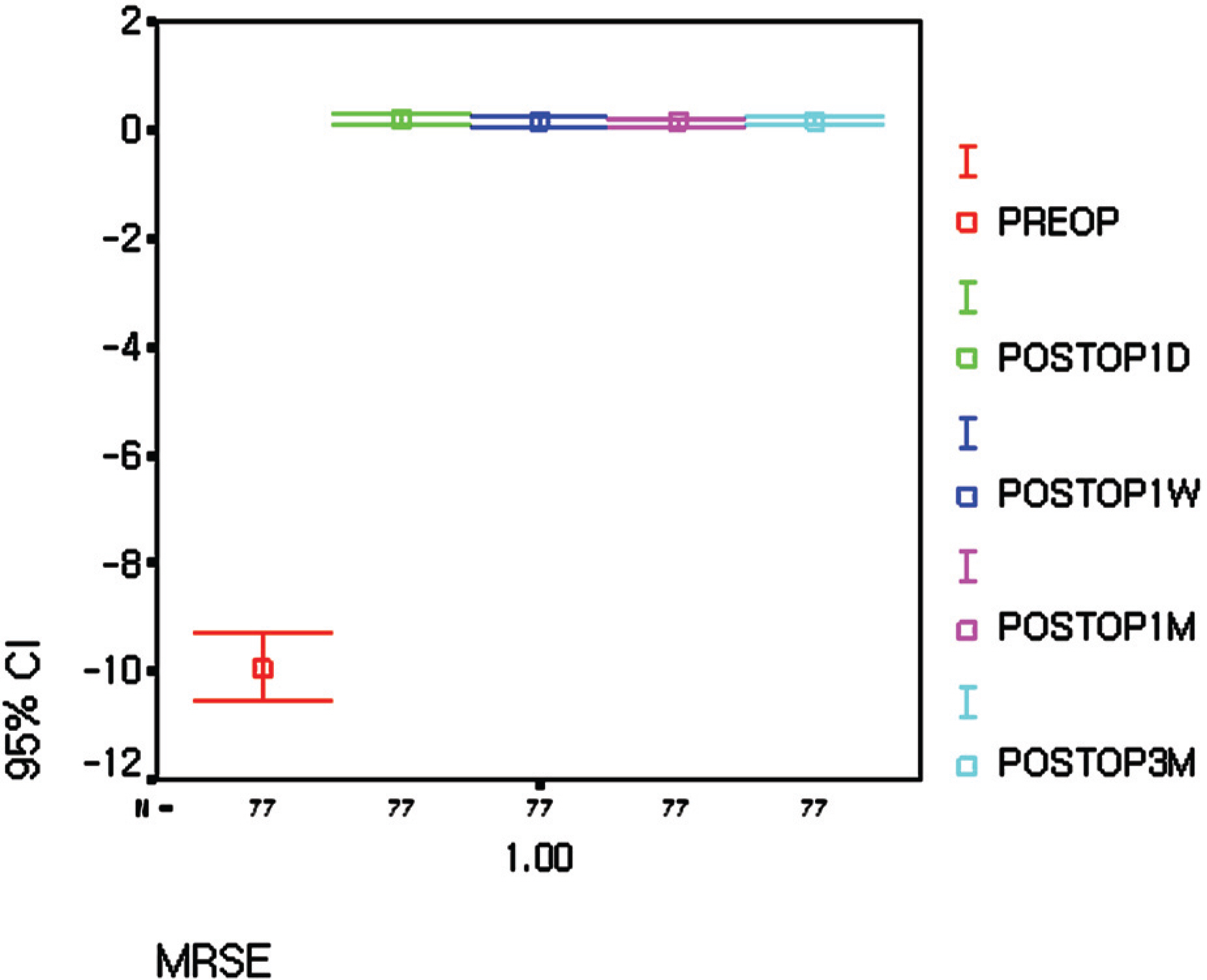
Figure 6. Spherical equivalent (MRSE=manifest refraction spherical equivalent).
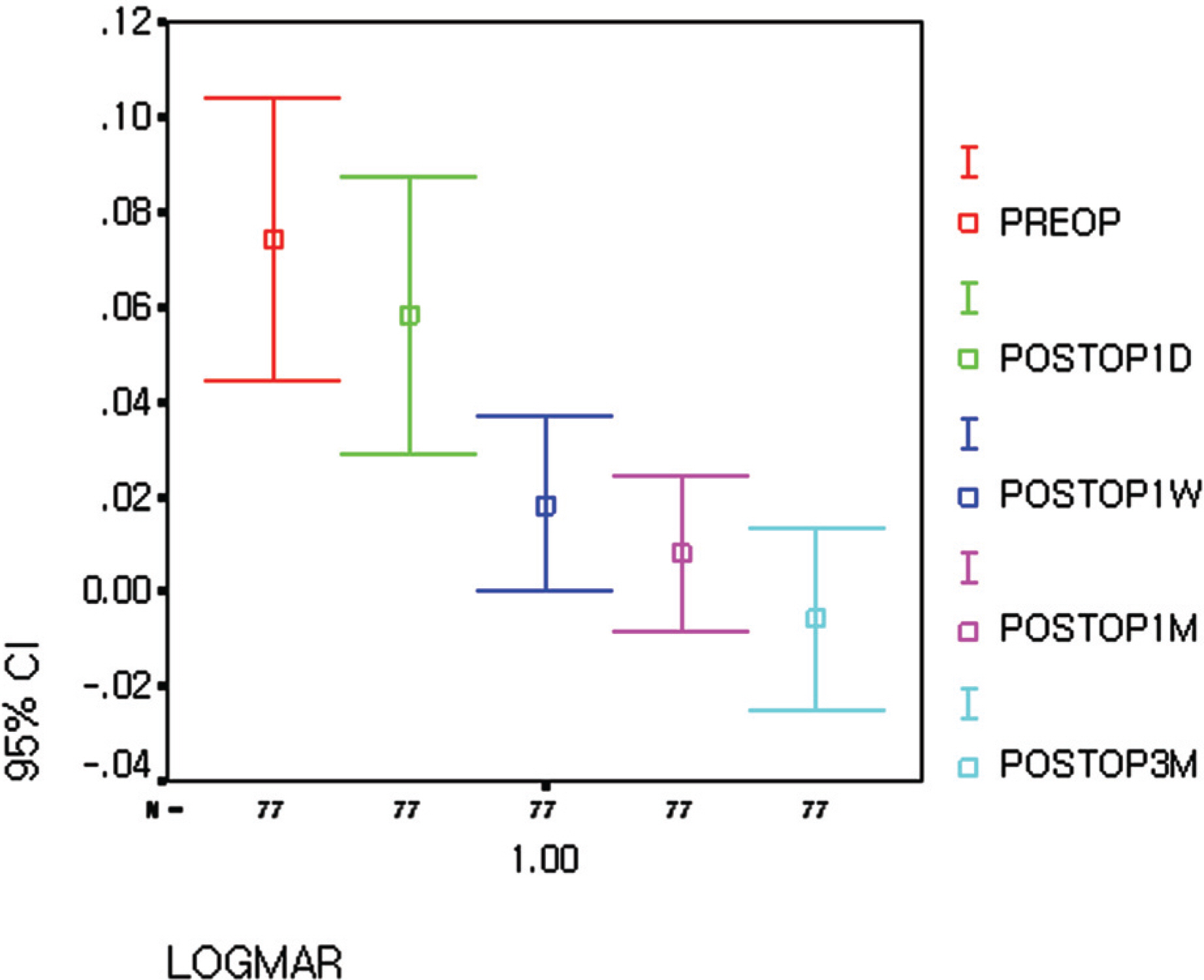
Figure 7. Best spectacle corrected visual acuity.
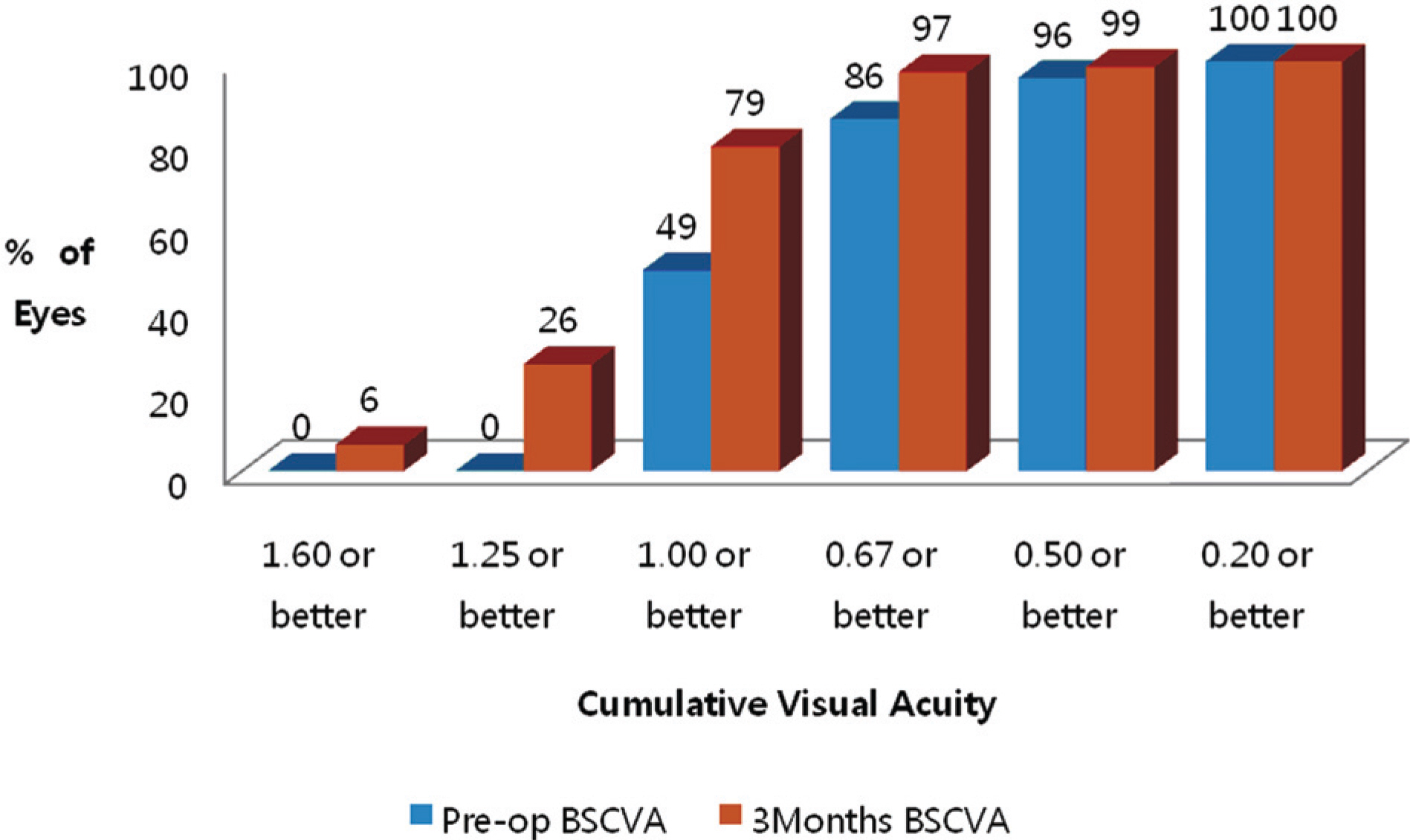
Figure 8. Preoperative (pre-op) versus 3-month post-operative best spectacle-corrected visual acuity (BSCVA) for the Toric Implantable Collamer Lens cohort.
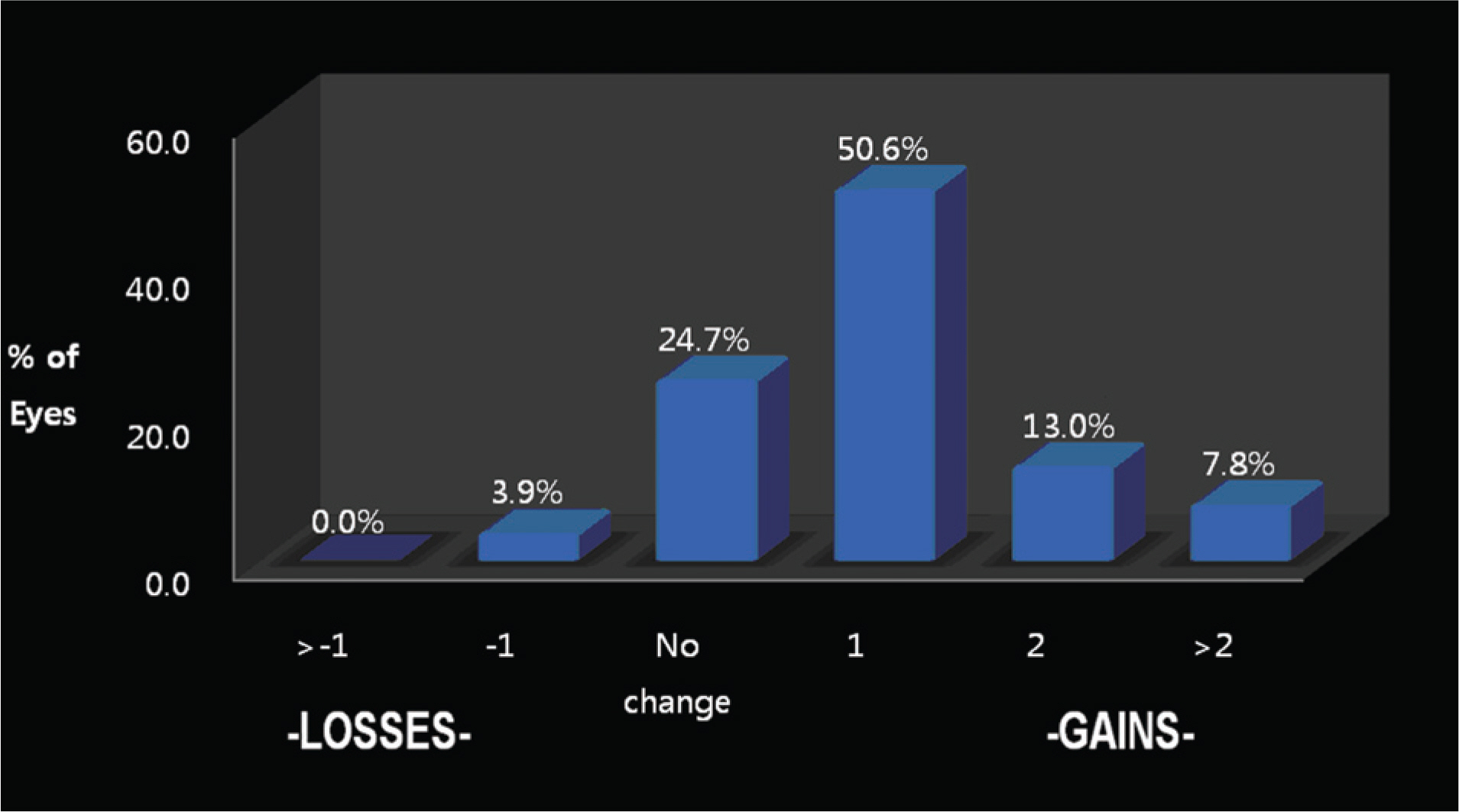
Figure 9. BSCVA line changes Preoperative versus 3-month postoperative line change in best spectacle-corrected visual acuity (BSCVA) for the Toric Implantable Collamer Lens cohort.
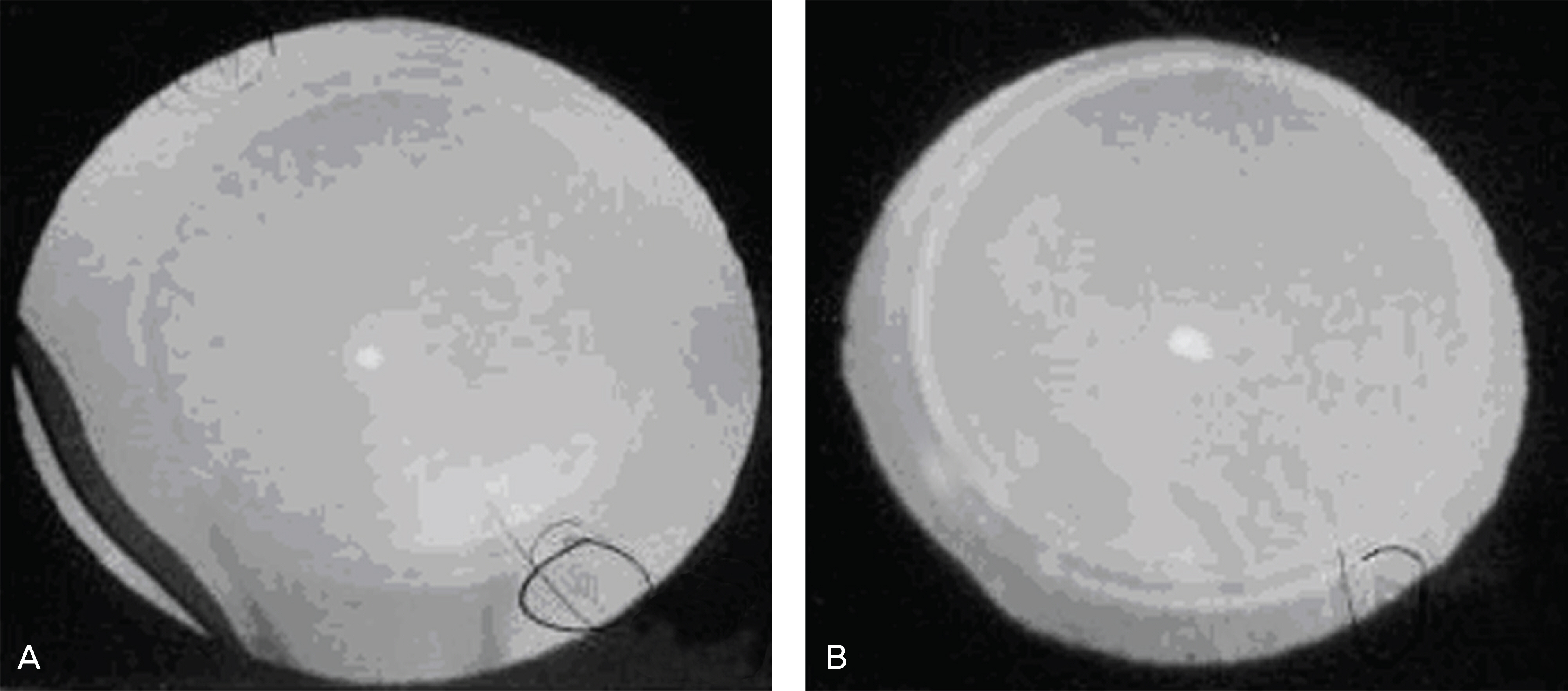
Figure 10. Scheimpflug photographs shows rotation of ICL. (A) First attack of rotation, postoperative 130 days. The rotation is about 45° clockwise from the initial position. (B) Second attack of rotation, postoperative 60 days after correction. The rotation is about the same as in the first attack.

Figure 11. Time sequence displacement of Toric ICL during surgical procedure that have rotational problem after surgery. (A) Axis alignment. (B) 5°clockwise rotation from the axis marker. (C) Correction of the misalignment by Vukich ICL manipulator during surgery. (D) At the end of the surgery, there was still 5° clockwise tilting even after repeated axis alignment.
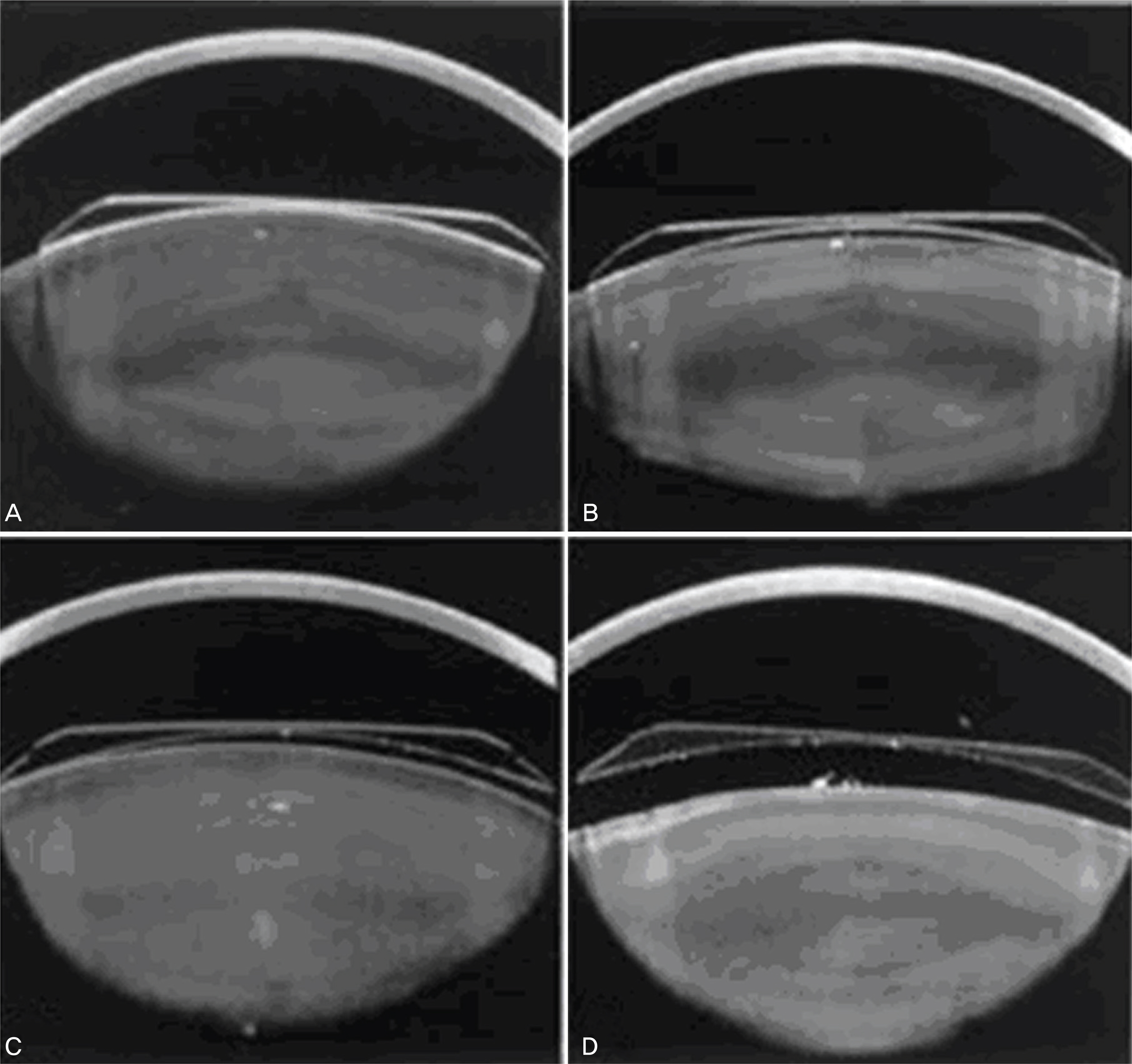
Figure 12. Four forms of vaulting as visualized with the Scheimpflug camera. (A) No central vaulting and no peripheral vaulting. (B) Low central vaulting and no peripheral vaulting. (C) Moderate central vaulting and partial/asymmetrical peripheral vaulting. (D) Marked central vaulting and complete peripheral vaulting.
Cited by 4 articles
-
Intraindividual Comparison of ICL and Toric ICL Implantation in the Correction of High Myopia With Astigmatism
Sang Youp Han, Sang Jung Moon, Ho Soong Kim, Tae Hun Lee, Kyung Hun Lee
J Korean Ophthalmol Soc. 2010;51(6):802-808. doi: 10.3341/jkos.2010.51.6.802.The Benefits of One Day, One Eye Surgery in Bilateral ICL Implantation
Wook Kyum Kim, Eun Young Cho, Hee Sun Kim, Deok Su Kim, Jin Kuk Kim
J Korean Ophthalmol Soc. 2013;54(7):1019-1024. doi: 10.3341/jkos.2013.54.7.1019.Clinical Outcomes of Beveled, Full Thickness Astigmatic Keratotomy
Bu Ki Kim, Su Joung Mun, Dae Gyu Lee, Young Taek Chung
J Korean Ophthalmol Soc. 2015;56(8):1160-1169. doi: 10.3341/jkos.2015.56.8.1160.Short-term Clinical Outcomes of Implantable Collamer Lens Implantation with Simultaneous Full Thickness Astigmatic Keratotomy
Buki Kim, Sujoung Mun, Hyuntae Choi, Youngtaek Chung
J Korean Ophthalmol Soc. 2017;58(8):916-923. doi: 10.3341/jkos.2017.58.8.916.
Reference
-
References
1. Tahzib NG, Cheng YY, Nuijts RM. Three-year follow-up analysis of Artisan toric lens implantation for correction of postkeratoplasty ametropia in phakic and pseudophakic eyes. Ophthalmology. 2006; 113:976–84.
Article2. Bartels MC, Saxena R, van den Berg TJ, et al. The influence of incision-induced astigmatism and axial lens position on the correction of myopic astigmatism with the Artisan toric phakic intraocular lens. Ophthalmology. 2006; 113:1110–7.
Article3. Gimbel HV, Ziemba SL. Management of myopic astigmatism with phakic intraocular lens implantation. J Cataract Refract Surg. 2002; 28:883–6.
Article4. Bartels MC, Santana NT, Budo C, et al. Toric phakic intraocular lens for the correction of hyperopia and astigmatism. J Cataract Refract Surg. 2006; 32:243–9.
Article5. Bartels MC, van Rij G, Luyten GP. Implantation of a toric phakic intraocular lens to correct high corneal astigmatism in a patient with bilateral marginal corneal degeneration. J Cataract Refract Surg. 2004; 30:499–502.
Article6. Dick HB, Alio J, Bianchetti M, et al. Toric phakic intraocular lens. European multicenter study. Ophthalmology. 2003; 110:150–62.7. Guell JL, Vazquez M, Malecaze F, et al. Artisan toric phakic intraocular lens for the correction of high astigmatism. Am J Ophthalmol. 2003; 136:442–7.8. Lee SY, Cheon HJ, Baek TM, Lee KH. Implantable contact lens to correct high myopia. J Korean Ophthalmol Soc. 2000; 41:1515–22.9. Chun YS, Lee JH, Lee JM, et al. Outcomes after implantable contact lens for moderate to high myopia. J Korean Ophthalmol Soc. 2004; 45:480–9.10. Han SY, Lee KH. Long term effect of ICL implantation to treat high myopia. J Korean Ophthalmol Soc. 2007; 48:465–72.11. Sanders DR, Brown DC, Martin RG, et al. Implantable contact lens for moderate to high myopia: phase I FDA clinical study with 6 month follow-up. J Cataract Refract Surg. 1998; 24:607–11.12. Sanders DR, Vukich JA, Doney K, Gaston M. Implantable Contact Lens in Treatment of Myopia Study Group. U.S. Food and Drug administration clinical trial of the implantable contact lens for moderate to high myopia. Ophthalmology. 2003; 110:255–66.13. Sanders DR, Schneider D, Martin RG, et al. Toric Implantable Collamer Lens for Moderate to High Myopic Astigmatism. Ophthalmology. 2007; 114:54–61.
Article14. ICL in Treatment of Myopia (ITM) Study Group. U.S. Food and Drug Administration clinical trial of the implantable contact lens for moderate to high myopia. Three-year follow-up. Ophthalmology. 2004; 111:1683–92.15. Jimenez-Alfaro I, Benitez del Castillo JM, Garcia-Feijoo J, et al. Safety of posterior chamber phakic intraocular lenses for the correction of high myopia. Anterior segment changes after posterior chamber phakic intraocular lens implantation. Ophthalmology. 2001; 108:90–9.16. Arne JL, Lesueur LC. Phakic posterior chamber lenses for high myopia: functional and anatomical outcomes. J Cataract Refract Surg. 2000; 26:369–74.
Article17. Gonvers M, Othenin-Girard P, Barnet C, Sickenberg M. Implantable contact lens for moderate to high myopia: short-term follow-up of 2 models. J Cataract Refract Surg. 2001; 27:380–8.18. Menezo JL, Peris-Martinez C, Cisneros A, Martinez-Costa R. Posterior chamber phakic intraocular lenses to correct high myopia: a comparative study between STAAR and Adatomed models. J Refract Surg. 2001; 17:32–42.
Article19. Pesando PM, Ghiringhello MP, Tagliavacche P. Posterior chamber collamer phakic intraocular lens for myopia and hyperopia. J Refract Surg. 1999; 15:415–23.20. Assetto V, Benedetti S, Pesando P. Collamer intraocular contact lens to correct high myopia. J Cataract Refract Surg. 1996; 22:551–6.
Article21. Zaldivar R, Davidorf JM, Oscherow S. Posterior chamber phakic intraocular lens for myopia of –8 to −19 diopters. J Refract Surg. 1998; 14:294–305.
Article22. BenEzra D, Cohen E, Karshai I. Phakic posterior chamber intraocular lens for the correction of anisometropia and treatment of amblyopia. Am J Ophthalmol. 2000; 130:292–6.
Article23. Fink AM, Gore C, Rosen E. Cataract development after implantation of the Staar Collamer posterior chamber phakic lens. J Cataract Refract Surg. 1999; 25:278–82.24. Kaya V, Kevser MA, Yilmaz OF. Phakic posterior chamber plate intraocular lenses for high myopia. J Refract Surg. 1999; 15:580–5.25. Rosen E, Gore C. Staar Collamer posterior chamber phakic intraocular lens to correct myopia and hyperopia. J Cataract Refract Surg. 1998; 24:596–606.
Article26. Durrie DS, Lesher MP, Cavanaugh TB. Classification of variable clinical response after photorefractive keratectomy for myopia. J Refract Surg. 1995; 11:341–7.
Article27. Sanders DR, Grabow HB, Shepherd J, Raanan MR. STAAR AA 4203T Toric Silicone IOL. Martin RG, Gillis JP, Sanders DR, editors. Foldable Intraocular Lenses. Thorofare, NJ: SLACK Inc.;1993. v. 1. chap.p. 14.28. Fechner PU. Cataract formation with a phakic IOL (letter to eheditor) J Caratact Refract Surg. 1999; 25:461.29. Gonvers M, Bornet C, Othenin-Girard P. Implantable contact lens for moderate to high myopia relationship of vaulting to cataract formation. J Caratact Refract Surg. 2003; 29:918–24.30. Cho SH, Park SH, Joo CH. A Case of High Myopic Astigmatism Corrected with a Toric Intraocular Lens. J Korean Ophthalmol Soc. 2007; 48:1281–4.
Article31. Varley GA, Huang D, Rapuano CJ, et al. LASIK for hyperopia, hyperopic astigmatism, and mixed astigmatism. (Ophthalmic Technology Assessment) A report by the American Academy of Ophthalmology. Ophthalmology. 2004; 111:1604–1617.32. Geggel HS, Talley AR. Delayed onser keratectasia following laser in situ keratomileusis and photorefractive keratecotmh. Ophthalmology. 2000; 107:640–52. 33.33. Holladay JT, Dudeja KR, Chang J. Functional vision and corneal changes after laser in situ keratoemiluesis determined by contrast sensitivity, glare testing, and corneal topography. J Cataract Refract Surg. 1999; 25:663–9.34. Lyle WA, Jin GJ. Laser in situ keratomileusis with the VISK star laser for myopia over 10.0 dipoters. J Cataract Refract Surg. 2001; 27:1812–22.35. Goker S, Er H, Kahvecioglu C. Laser in situ keratomileusis to correct hyperopia from +4.25 to +8.00 diopters. J Refract Surg. 1998; 14:26–30.
Article36. Nagy ZZ, Munkácsy G, Popper M. Photorefractive keratectomy using the Meditec MEL 70 G-scan laser for hyperopia and hyperopic astigmatism. J Refract Surg. 2002; 18:542–50.
Article37. Richard LL, Douglas DK, Robert HO, Li W. Control of Astigmatism in the Cataract Patient. Natasha Andjelkovic, editor. Cataract surgery Technique, Complications, and Management. 2nd ed.Philadelphia: Elsevier;2004. chap.p. 22.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Short-term Clinical Outcomes of Implantable Collamer Lens Implantation with Simultaneous Full Thickness Astigmatic Keratotomy
- Rotational Stability after Toric Implantable Collamer Lens Implantation
- Partial Visual Rehabilitation Using a Toric Implantable Collamer Lens in a Patient with Keratoconus: A Case Report with 20 Months of Follow-up
- Long-term Clinical Outcomes of Implantable Collamer Lens
- Efficacy of Biometry Using Swept-source Optical Coherence Tomography for Posterior Chamber Phakic Intraocular Lens Implantation
