J Korean Surg Soc.
2012 Jul;83(1):50-55. 10.4174/jkss.2012.83.1.50.
Pneumocystis carinii pneumonia in gastric cancer patients without acquired immune deficiency syndrome: 3 cases report and literature review
- Affiliations
-
- 1Department of Hematooncology, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea.
- 2Department of Infectious Diseases, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea.
- 3Department of Surgery, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea. yoomw@kuh.ac.kr
- KMID: 2212279
- DOI: http://doi.org/10.4174/jkss.2012.83.1.50
Abstract
- Pneumocystis carinii pneumonia (PCP) has rarely been reported in solid tumor patients. It is a well-known complication in immunosuppressed states including acquired immune deficiency syndrome and hematologic malignancy. PCP has been reported in solid tumor patients who received long-term steroid treatment due to brain or spinal cord metastases. We found 3 gastric cancer patients with PCP, who received only dexamethasone as an antiemetic during chemotherapy. The duration and cumulative dose of dexamethasone used in each patient was 384 mg/48 days, 588 mg/69 days, and 360 mg/42 days, respectively. These cases highlight that the PCP in gastric cancer patients can successfully be managed through clinical suspicion and prompt treatment. The cumulative dose and duration of dexamethasone used in these cases can be basic data for risk of PCP development in gastric cancer patients during chemotherapy.
MeSH Terms
Figure
-
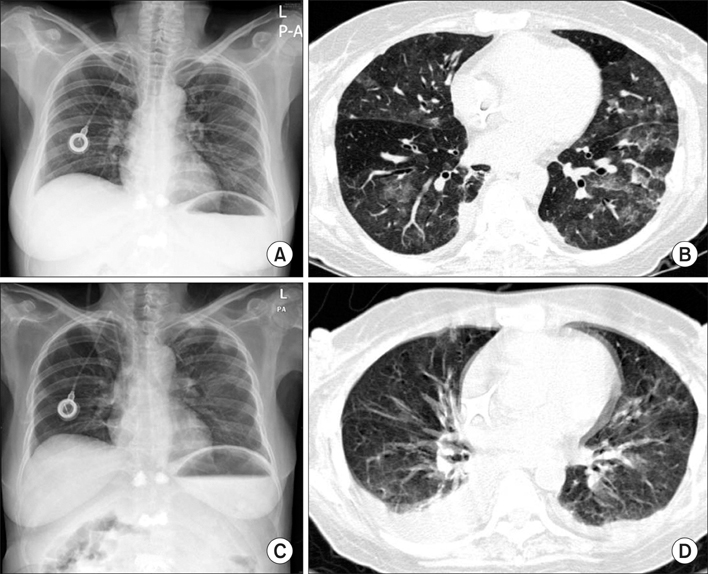
Fig. 1 Chest posterior-anterior view and computed tomography (CT) of patient 1. A and B is the chest X-ray and CT of before anti-pneumocystis carinii pneumonia (PCP) treatment and C and D is that of after anti-PCP treatment respectively.

Fig. 2 Chest posterior-anterior view and computed tomography (CT) of patient 2. A and B is the chest X-ray and CT of before anti-pneumocystis carinii pneumonia (PCP) treatment and C and D is that of after anti-PCP treatment respectively.
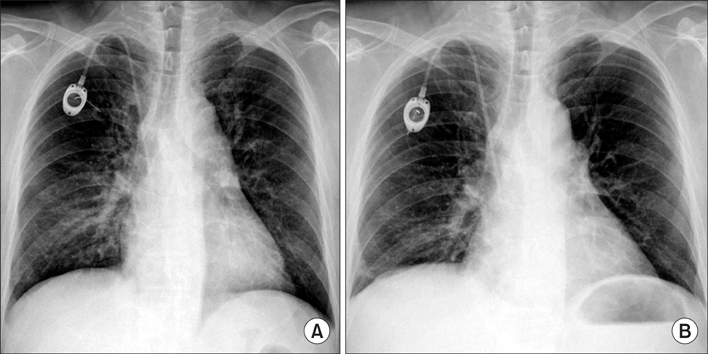
Fig. 3 Chest posterior-anterior view of patient 3. A and B is the chest X-ray of before anti-pneumocystis carinii pneumonia (PCP) treatment and that of after anti-PCP treatment respectively.
Reference
-
1. Arend SM, Kroon FP, van't Wout JW. Pneumocystis carinii pneumonia in patients without AIDS, 1980 through 1993: an analysis of 78 cases. Arch Intern Med. 1995. 155:2436–2441.2. Gal AA, Plummer AL, Langston AA, Mansour KA. Granulomatous Pneumocystis carinii pneumonia complicating hematopoietic cell transplantation. Pathol Res Pract. 2002. 198:553–558.3. Varthalitis I, Aoun M, Daneau D, Meunier F. Pneumocystis carinii pneumonia in patients with cancer: an increasing incidence. Cancer. 1993. 71:481–485.4. Barbounis V, Aperis G, Gambletsas E, Koumakis G, Demiris M, Vassilomanolakis M, et al. Pneumocystis carinii pneumonia in patients with solid tumors and lymphomas: predisposing factors and outcome. Anticancer Res. 2005. 25(1B):651–655.5. Walzer P. Mandell GL, Douglas RG, Bennett JE, editors. Pneumocystis carinii. Principles and practice of infectious disease. 1989. New York: Churchill Livingstone;2103–2110.6. Jacobs JA, Dieleman MM, Cornelissen EI, Groen EA, Wagenaar SS, Drent M. Bronchoalveolar lavage fluid cytology in patients with Pneumocystis carinii pneumonia. Acta Cytol. 2001. 45:317–326.7. Limper AH, Offord KP, Smith TF, Martin WJ 2nd. Pneumocystis carinii pneumonia: differences in lung parasite number and inflammation in patients with and without AIDS. Am Rev Respir Dis. 1989. 140:1204–1209.8. Shelhamer JH, Gill VJ, Quinn TC, Crawford SW, Kovacs JA, Masur H, et al. The laboratory evaluation of opportunistic pulmonary infections. Ann Intern Med. 1996. 124:585–599.9. Thomas CF Jr, Limper AH. Pneumocystis pneumonia: clinical presentation and diagnosis in patients with and without acquired immune deficiency syndrome. Semin Respir Infect. 1998. 13:289–295.10. Jordan K, Sippel C, Schmoll HJ. Guidelines for antiemetic treatment of chemotherapy-induced nausea and vomiting: past, present, and future recommendations. Oncologist. 2007. 12:1143–1150.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Pneumocystis carinii Pneumonia in an Infant with Failure to Thrive
- Combined Pneumocystis Carinii Pneumonia and Miliary Tuberculosis in a Patient with AIDS
- A Case of Pneumocystis Carinii Pneumonia in a Patient with Felty's Syndome
- Two Autopsy Cases of Pneumocystis Carinii Pneumonia
- A Case of Pneumocystis carinii Pneumonia with Febrile Neutropenia in Acute Lymphoblastic Leukemia
