Experience and analysis of level VII cervical lymph node metastases in patients with papillary thyroid carcinoma
- Affiliations
-
- 1Department of Surgery, Kosin University College of Medicine, Busan, Korea. gskjh@hanafos.com
- 2Department of Internal Medicine, Kosin University College of Medicine, Busan, Korea.
- KMID: 2212154
- DOI: http://doi.org/10.4174/jkss.2011.80.5.307
Abstract
- PURPOSE
Papillary thyroid cancer with level VII (anterior superior mediastinal lymph nodes) lymph node metastasis belongs to Stage IV a according to the Americal Joint Committee on Cancer cancer staging. The aim of our study was to identify clinicopathologic factors that are related to level VII cervical lymph node metastasis and to suggest recommendations for level VII dissection.
METHODS
We reviewed 195 patients with papillary thyroid carcinoma who had their initial operation containing level VII dissection from April 2006 to June 2007. Level VII dissection involved lymph nodes in the anterior superior mediastinum and tracheoesophageal grooves, extending from the suprasternal notch to the innominate artery. Clinicophathologic factors, such as gender, age and lateral neck metastasis, related to Level VII metastasis were analyzed by tumor size, multifocality of tumor, extrathyroidal extension and lymphovascular invasion.
RESULTS
Nine (4.6%) of 195 patients with papillary thyroid carcinoma had level VII metastasis. Clinicopathologic factors that were related to level VII metastasis included lateral neck metastasis (P < 0.01), tumor size (P < 0.01) and lymphovascular invasion (P < 0.05).
CONCLUSION
If preoperatively, the tumor size is over 1.5 cm, or there is lateral neck metastasis, level VII dissection must be considered. If there is lymphovascular invasion pathologic findings postoperatively, special attention should be paid for detection of level VII recurrence.
MeSH Terms
Figure
-
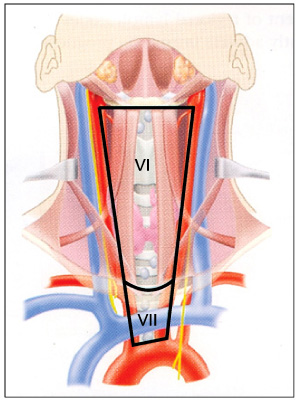
Fig. 1 Anatomical boundaries of nodal levels VI (central compartment group) and Vll (superior mediastinal group) (reprinted from Shah JP, Patel SG. Head and neck surgery and oncology. 3rd ed. London: Mosby; 2002. p.355, with permission of Elsevier.) [10].
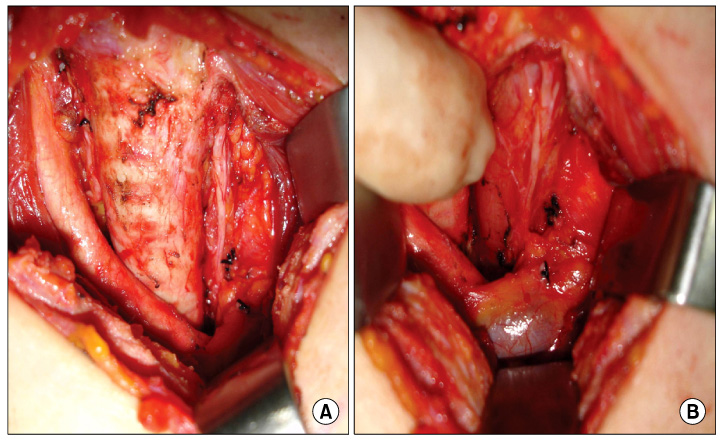
Fig. 2 The surgical field following level Vll dissection. (A) The right innominate artery was dissected free from the level Vll lymph nodes. (B) The left innominate vein was dissected from the level Vll lymph nodes and the left common carotid artery was retracted laterally with a long-arm retractor.

Fig. 3 (A) Right thyroid lobectomy, along with level Vl and Vll dissection was performed as en bloc dissection. (B) We separated level Vll lymph nodes from thyroid and level Vl lymph nodes after resection.
Reference
-
1. McConahey WM, Hay ID, Woolner LB, van Heerden JA, Taylor WF. Papillary thyroid cancer treated at the Mayo Clinic, 1946 through 1970: initial manifestations, pathologic findings, therapy, and outcome. Mayo Clin Proc. 1986. 61:978–996.2. Rossi RL, Cady B, Silverman ML, Wool MS, Horner TA. Current results of conservative surgery for differentiated thyroid carcinoma. World J Surg. 1986. 10:612–622.3. Hay ID, Bergstralh EJ, Goellner JR, Ebersold JR, Grant CS. Predicting outcome in papillary thyroid carcinoma: development of a reliable prognostic scoring system in a cohort of 1779 patients surgically treated at one institution during 1940 through 1989. Surgery. 1993. 114:1050–1057.4. Sato N, Oyamatsu M, Koyama Y, Emura I, Tamiya Y, Hatakeyama K. Do the level of nodal disease according to the TNM classification and the number of involved cervical nodes reflect prognosis in patients with differentiated carcinoma of the thyroid gland? J Surg Oncol. 1998. 69:151–155.5. Mazzaferri EL, Jhiang SM. Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am J Med. 1994. 97:418–428.6. Scheumann GF, Gimm O, Wegener G, Hundeshagen H, Dralle H. Prognostic significance and surgical management of locoregional lymph node metastases in papillary thyroid cancer. World J Surg. 1994. 18:559–567.7. Hughes CJ, Shaha AR, Shah JP, Loree TR. Impact of lymph node metastasis in differentiated carcinoma of the thyroid: a matched-pair analysis. Head Neck. 1996. 18:127–132.8. Lundgren CI, Hall P, Dickman PW, Zedenius J. Clinically significant prognostic factors for differentiated thyroid carcinoma: a population-based, nested case-control study. Cancer. 2006. 106:524–531.9. Greene FL, Page DL, Fleming ID, Fritz AG, Balch CM, Haller DG, et al. AJCC cancer staging manual. 2002. 6th ed. New York: Springer-Verlag;77–87.10. Shah JP, Patel SG. Head and neck surgery and oncology. 2002. 3rd ed. London: Mosby;355.11. Grebe SK, Hay ID. Prognostic factors and management in thyroid cancer--consensus or controversy? West J Med. 1996. 165:156–157.12. Clark OH. Predictors of thyroid tumor aggressiveness. West J Med. 1996. 165:131–138.13. Robbins KT, Medina JE, Wolfe GT, Levine PA, Sessions RB, Pruet CW. Standardizing neck dissection terminology. Official report of the Academy's Committee for Head and Neck Surgery and Oncology. Arch Otolaryngol Head Neck Surg. 1991. 117:601–605.14. Robbins KT, Clayman G, Levine PA, Medina J, Sessions R, Shaha A, et al. Neck dissection classification update: revisions proposed by the American Head and Neck Society and the American Academy of Otolaryngology-Head and Neck Surgery. Arch Otolaryngol Head Neck Surg. 2002. 128:751–758.15. Goropoulos A, Karamoshos K, Christodoulou A, Ntitsias T, Paulou K, Samaras A, et al. Value of the cervical compartments in the surgical treatment of papillary thyroid carcinoma. World J Surg. 2004. 28:1275–1281.16. Hay ID, Thompson GB, Grant CS, Bergstralh EJ, Dvorak CE, Gorman CA, et al. Papillary thyroid carcinoma managed at the Mayo Clinic during six decades (1940-1999): temporal trends in initial therapy and long-term outcome in 2444 consecutively treated patients. World J Surg. 2002. 26:879–885.17. White ML, Gauger PG, Doherty GM. Central lymph node dissection in differentiated thyroid cancer. World J Surg. 2007. 31:895–904.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Pattern of Cervical Lymph Node Metastases in Papillary Thyroid Cancer
- Papillary Thyroid Cancer Arising in Lateral Aberrant Thyroid Presenting with Multiple Metastases
- Pattern of Lateral Neck Metastasis and Predictors of Level V Metastasis in Papillary Thyroid Carcinoma
- Retropharyngeal Lymph Node Metastasis from Thyroid Papillary Carcinoma with Airway Obstruction
- Pattern of Cervical Neck Lymph Node Metastasis in Papillary Thyroid Carcinoma according to Tumor Size
