The Changes in Macular Thickness after Phacoemulsification in Patients with Non-diabetes and Nonproliferative Diabetic Retinopathy
- Affiliations
-
- 1Department of Ophthalmology, Chungnam National University College of Medicine, Daejeon, Korea. shchoi@cnu.ac.kr
- KMID: 2211183
- DOI: http://doi.org/10.3341/jkos.2008.49.1.57
Abstract
-
PURPOSE: To compare the changes in macular thickeness between non-diabetic group and a mild or moderate nonproliferative diabetic retinopathy group after phacoemulsification.
METHODS
This study consisted of 32 eyes of 22 patients who underwent phacoemulsification. The non-diabetic group included 20 eyes of 15 patients; the diabetic group (mild or moderate nonproliferative diabetic retinopathy) included 12 eyes of 7 patients. Macular thickness using optical coherence tomography (OCT) and corrected visual acuity were measured before surgery and 1 day, 1 week, 1 month, 2 months, 6 months and 12 months after surgery.
RESULTS
In the non-diabetic group, the macular thickness increased by 2.8+/-4.2% at 1 week, 5.9+/-4.5% at 1 month, 4.8+/-3.8% at 2 months, 0.6+/-0.8% at 6 months, and -0.3+/-1.2% at 12 months after surgery, while it increased by 4.8+/-5.0% at 1 week, 11.1+/-5.2% at one month, 9.9+/-6.0% at two months, 8.1+/-4.6% at 6 months, 3.9+/-3.5% at 12 months in the diabetic group. The increased amount of macular thickness was significantly higher in the diabetic group than in the non-diabetic group at 1 month, 2 months, 6 months, and 12 months. Visual acuity was not significantly different between the diabetic and non-diabetic groups. In the non-diabetic group, 2 months after the operation, LogMAR below 0.02 (Snellen 0.95) were remained with best corrected visual acuity. Similarly to non-diabetic patients, diabetic patients needed 12 months to reach best corrected visual acuity.
CONCLUSIONS
Macular thickness increased in both diabetic and non-diabetic groups after phacoemulsification, and the increased amount of macular thickness was significantly greater and lasted longer in the diabetic group compared with the non-diabetic group. In cases of mild or moderate nonproliferative diabetic retinopathy, macular thickness change due to cataract surgery did not influence visual acuity.
Keyword
MeSH Terms
Figure
-
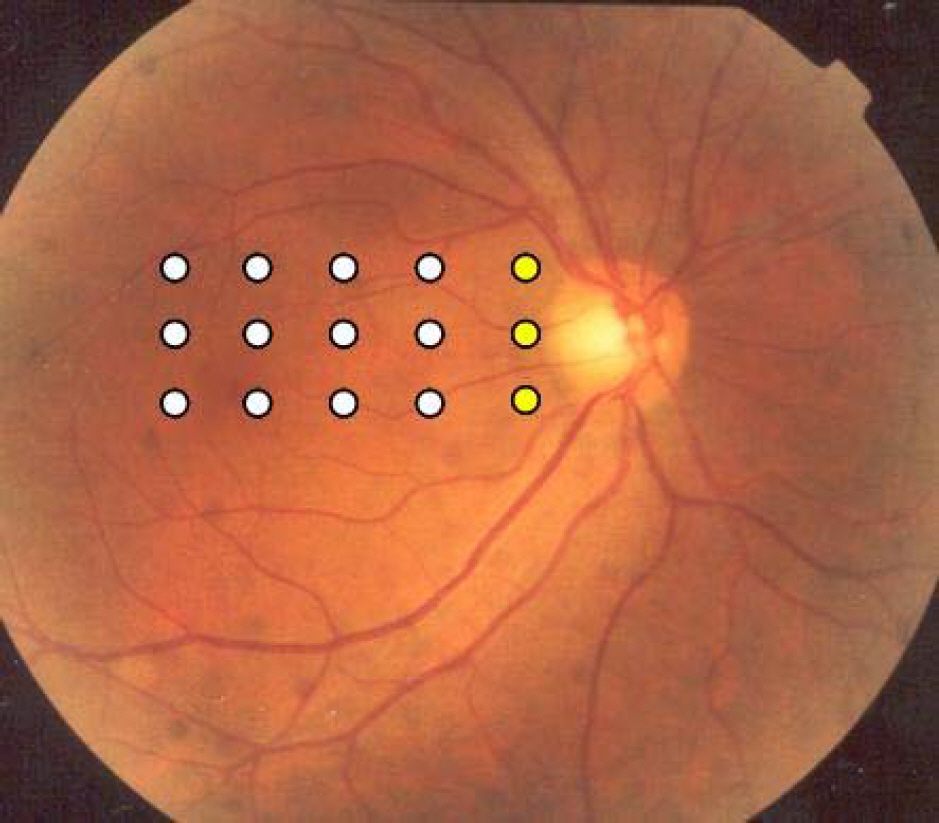
Figure 1. Location of 3 linear OCT scans preoperative and postoperatively. The first scan is extended from temporal edge of nerve head to 4.0 mm temporally. The other two scans locate parallelly to the first line, at the level of the upper and lower margin of the optic nerve head. Retinal thicknesses of 4 mm scan are measured from 5 different points having 1 mm distance away. Total three scans are taken, therefore 15 points are measured and recorded. Among these, 3 points, which are closest to the optic disc, are excluded from calculating the average of retinal thickness, so the 12 points are selected to calculate the average.

Figure 2. Change of mean retinal thickness (µm); before surgery, postoperative 1 day, 1 week, 1 month, 2 months, 6 months and 12 months in non-diabetic and diabetic groups after phacoemulsification. The mean retinal thickness between non-diabetic group and diabetic group is not statistically different at all time intervals.
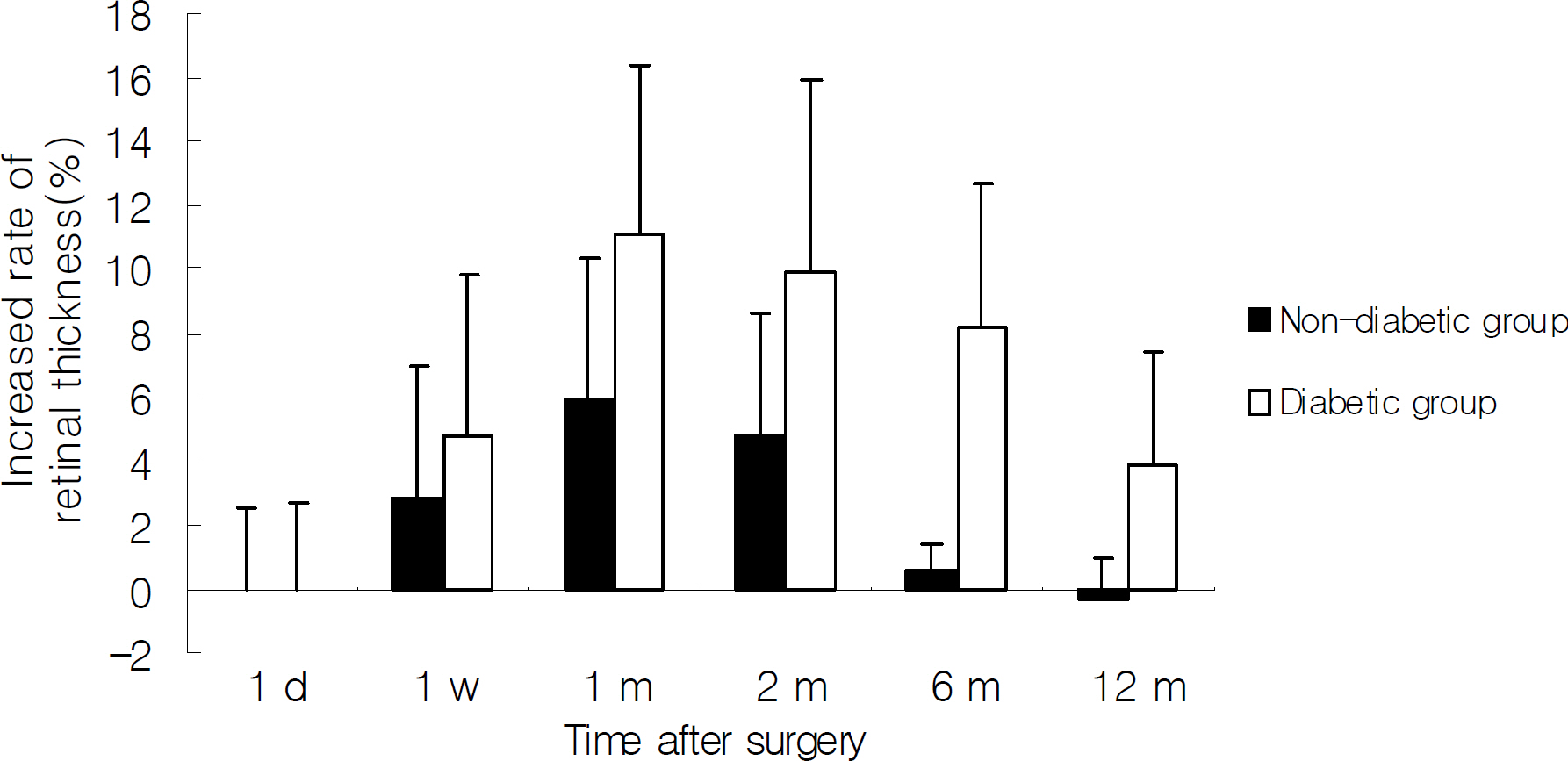
Figure 3. Comparison of percentage increase of retinal thickness between preoperative value and postoperative 1 day, 1 week, 1 month, 2 months, 6 months, 12 months respectively in non-diabetic and diabetic group after phacoemulsification. In non-diabetic group, percentage increase is statistically significant at 1 week, 1 month, and 2 months. In diabetic group, percentage increase is statistically significant at all time intervals.
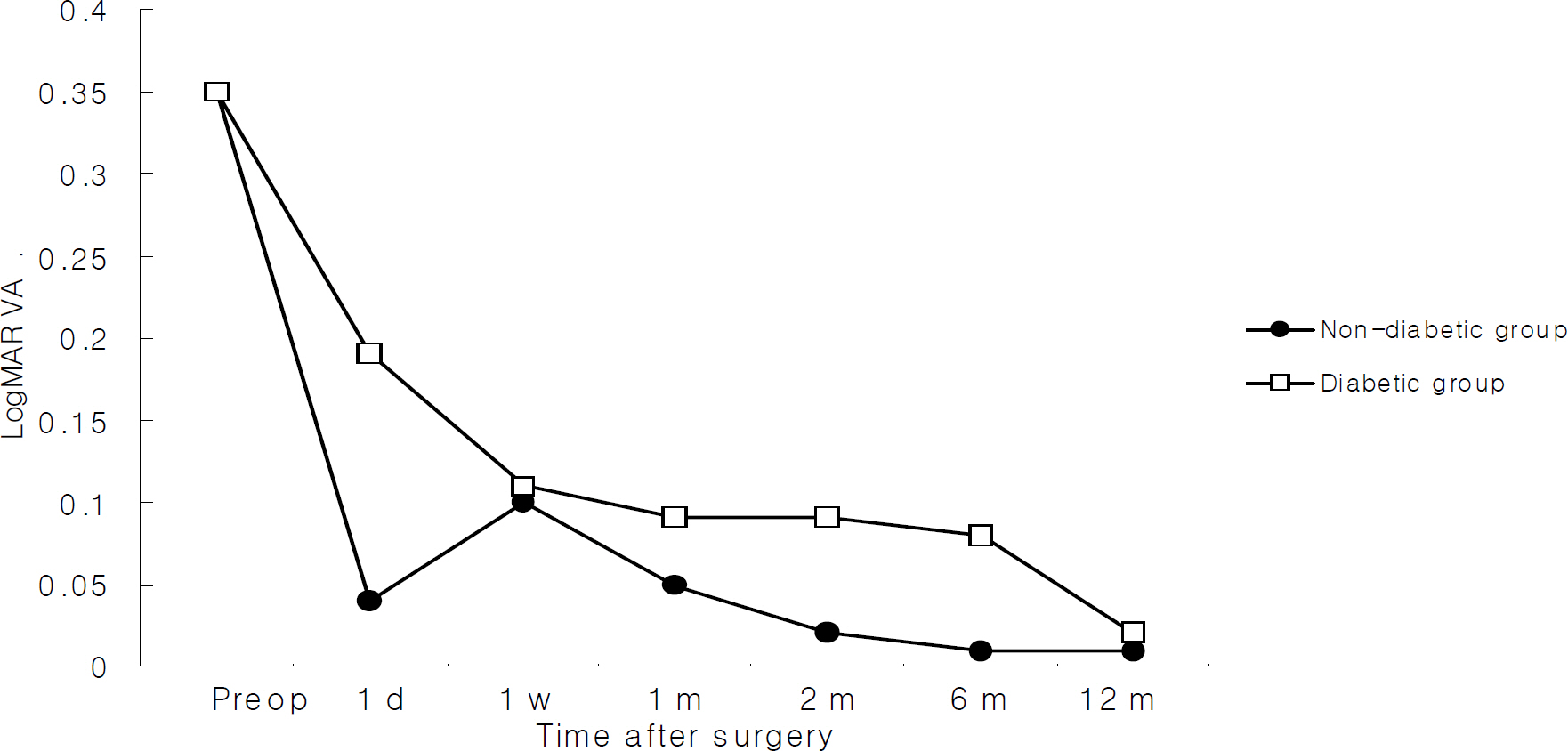
Figure 4. Change of best corrected visual acuity in LogMAR before and after phacoemulsification. In non-diabetic group, after 2 months of the operation, Log MAR below 0.02 (Snellen 0.95) are relatively remained with best corrected visual acuity. In diabetic group, it takes 12 months to reach the best corrected visual acuity, which is similar to non-diabetic group.
Cited by 1 articles
-
The Results of a Combination of Cataract Surgery and Intravitreal Bevacizumab Injection for Diabetic Macular Edema
Bu Ki Kim, Eui Yong Kweon, Dong Wook Lee, Min Ahn, Nam Chun Cho
J Korean Ophthalmol Soc. 2010;51(7):954-960. doi: 10.3341/jkos.2010.51.7.954.
Reference
-
References
1. Rossetti L, Autelitano A. Cystoid macular edema following cataract surgery. Curr Opin Ophthalmol. 2000; 11:65–72.
Article2. Powe NR, Schein OD, Gieser SC, et al. Synthesis of the literature on visual acuity and complications following cataract extraction and intraocular lens implantation. Arch Ophthalmol. 1994; 112:239–52.3. Riley AF, Malik TY, Grupcheva CN, et al. The Auckland cataract study: comorbidity, surgical techniques and clinical outcomes in a public hospital service. Br J Ophthalmol. 2002; 86:185–90.
Article4. Ursell PG, Spalton DJ, Whitcup SM. Cystoid macular oedema after phacoemulsification: relationship to blood aqueous barrier damage and visual acuity. J Cataract Refract Surg. 1999; 25:1492–7.5. Simon N, Andrew R, Hussain P, et al. Correlations between optical coherence tomography measurement of macular thickness and visual acuity after cataract extraction. Clin Experiment Ophthalmol. 2006; 34:124–9.6. Ching HY, Wong AC, Wong CC, et al. Cystoid macular oedema and changes in retinal thickness after phacoemulsifi cation with optical coherence tomography. Eye. 2006; 20:297–303.7. Ah-Fat FG, Sharma MK, Majid MA, Yang YC. Vitreous loss during conversion from conventional extracapsular cataract extraction to phacoemulsification. J Cataract Refract Surg. 1998; 24:801–5.
Article8. Henry MM, Henry LM. A possible cause of chronic cystic maculopathy. Ann Ophthalmol. 1977; 9:455–7.9. Irvine SR. A newly defined vitreous syndrome following cataract surgery interpreted according to recent concepts of the structure of the vitreous. Am J Ophthalmol. 1953; 36:599–619.10. Jampol LM, Sanders DR, Kraff MC. Prophylaxis and therapy of aphakic cystoid macular edema. Surv Ophthalmol. 1984; 28:535–9.
Article11. Dowler JG, Hykin PG, Lightman SL, Hamilton AM. Visual acuity following extracapsular cataract extraction in diabetes: a meta-analysis. Eye. 1995; 9:313–7.
Article12. Schatz H, Atienza D, McDonald HR, Johnson RN. Severe diabetic retinopathy after cataract surgery. Am J Ophthalmol. 1994; 117:314–21.
Article13. Pollack A, Leiba H, Bukelman A, Oliver M. Cystoid macular oedema following cataract extraction in patients with diabetes. Br J Ophthalmol. 1992; 76:221–4.
Article14. Dowler JG, Sehmi KS, Hykin PG, Hamilton AM. The natural history of macular edema after cataract surgery in diabetes. Ophthalmology. 1999; 106:663–8.
Article15. Smith RE, Godfrey WA, Kimura SJ. Complications of chronic cyclitis. Am J Ophthalmol. 1976; 82:277–82.
Article16. Ursell PG, Spalton DJ, Whitcup SM, Nussenblatt RB. Cystoid macular edema after phacoemulsification: Relationship to blood ?aqueous barrier damage and visual acuity. J Cataract Refract Surg. 1999; 25:1492–7.17. Benson WE, Brown GC, Tasman W, et al. Extracapsular cataract extraction with placement of a posterior chamber lens in patients with diabetic retinopathy. Ophthalmology. 1993; 100:730–8.
Article18. Cheng H, Franklin SL. Treatment of cataracts in diabetics with and without retinopathy. Eye. 1988; 2:607–14.19. Cunliffe IA, Flanagan DW, George ND, et al. Extracapsular cataract surgery in patients with lens implantation in patients with and without proliferative retinopathy. Br J Ophthalmol. 1991; 75:9–12.20. Hykin PG, Gregson RM, Stevens JD, Hamilton AM. Extracapsular cataract extraction in proliferative diabetic retinopathy. Ophthalmology. 1993; 100:394–9.
Article21. Jaffe GJ, Burton TJ. Progression of nonproliferative diabetic retinopathy following cataract extraction. Arch Ophthalmol. 1988; 106:745–9.
Article22. Jaffe GJ, Burton TC, Kuhn E, et al. Progression of nonproliferative daibetic retinopathy and visual outcome after extracapsular cataract extraction and intraocular lens implantation. Am J Ophthalmol. 1992; 114:448–56.23. Pollack A, Dotan S, Oliver M. Course of diabetic retinopathy following cataract surgery. Br J Ophthalmol. 1991; 75:2–8.
Article24. Pollack A, Dotan S, Oliver M. Progression of diabetic retinopathy after cataract extraction. Br J Ophthalmol. 1991; 75:547–51.
Article25. Miyak K. Indomethacin in the treatment of postoperative cystoid macular edema. Surv Ophthalmol. 1984; 28:554–68.26. Yannauzzi LA, Landau AN, Turtz AI. Incidence of aphakic cystoid macular edema with the use of topical indomethacin. Ophthalmology. 1981; 88:947–54.
Article27. Jung HJ, Hyun JH, Kim YI, et al. Normal Macular Thickness Measured Macular Mapping of OCT3. J Korean Ophthalmol Soc. 2004; 45:962–968.28. Neubauer AS, Pringlinger S, Ullrich S, et al. Comparison of foveal thickness measured with the retinal thickness analyzer and optical coherence tomography. Retina. 2001; 21:596–601.
Article29. Massin P, Vicat E, Haouchine B, et al. Reproducibility of retinal mapping using optical coherence tomography. Arch Ophthalmol. 2001; 119:135–42.
Article30. Matthias B, Ronald CG, Jeffrey ML, Robert R. Reproducibility of retinal thickness measurements in normal eyes using optical coherence tomography. Ophthalmic Surg Lasers. 1998; 29:280–5.31. Lee HS, Shin HH, Byun YJ. Retinal thickness after cataract surgery measured by optical coherence tomography. J Korean Ophthalmol Soc. 2004; 45:203–8.32. Kent D, Vinores SA, Campochiaro PA. Macular oedema: the role of soluble mediators. Br J Ophthalmol. 2000; 84:542–5.
Article33. Bazan NG. Metabolism of arachidonic acid in the retina and retinal pigment epithelium: biological effects of oxygenated metabolites of arachidonic acid. Prog Clin Biol Res. 1989; 312:15–37.34. Kim SJ, Equi R, Bressler NM. Analysis of macular edema after cataract surgery in patients with diabetes using optical coherence tomography. Ophthalmology. 2007; 114:881–9.
Article35. Diabetic Retinopathy Clinical Research Network. Browning DJ, Glassman AR, Aiello LP, et al. Relationship between optical coherence tomography-measured central thickness and visual acuity in diabetic macular edema. Ophthalmology. 2007; 114:525–36.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Quantitative Analysis of Macular Thickness with OCT Map
- Retinal Thickness After Cataract Surgery Measured by Optical Coherence Tomography
- Diurnal Variation of Macular Thickness in Diabetic Macular Edema
- Changes in Macular Thickness after Cataract Surgery According to Optical Coherence Tomography
- Influence of Phacoemulsification on the Progression of Diabetic Retinopathy
