J Korean Soc Spine Surg.
2010 Dec;17(4):164-168. 10.4184/jkss.2010.17.4.164.
The Influence of Cervical Spondylosis to Acute Cervical Spinal Cord Injury
- Affiliations
-
- 1Department of Orthopaedic Surgery, Chonnam National University Hospital, Korea. hyseo2001@hanmail.net
- KMID: 2209578
- DOI: http://doi.org/10.4184/jkss.2010.17.4.164
Abstract
- STUDY DESIGN: A retrospective study
OBJECTIVES
To examine the influence of cervical spondylosis on an acute cervical spinal cord injury. SUMMARY OF LITERATURE REVIEW: There are no reports on the relationship between cervical spondylosis and acute cervical spinal cord injuries.
MATERIALS AND METHODS
Twenty six patients who underwent operative treatment for acute cervical injuries with spinal cord injury were evaluated. The mean age and follow-up period was 58 years and 2.2 years, respectively. The evaluation was performed by examining the causes of the injuries, and the classification of fractures according to the presence of cervical spondylosis. This study compared the degrees of postoperative neurological recovery with motor index score in the groups with and without cervical spondylosis.
RESULTS
Cervical cord injuries were more prevalent in the group 60 years and older; 17 cases vs. 9 cases in the group under 60 years. Eleven (65%) and 6 (35%) cases in the group 60 years and older had sustained a high and low energy injury, respectively. In contrast, mostly high energy injuries (8 in 9 cases) were encountered in the group under 60 years of age. A low energy injury could cause a acute cervical cord injury in the group 60 years and older, who also had cervical spondylosis. In those cases, previous cervical spondylosis might be one of the etiologic factors.
CONCLUSIONS
The cases with cervical spondylosis in the group 60 years and older tended to show incomplete cord injury and good postoperative neurological recovery when they had sustained cervical cord injuries.
Figure
-
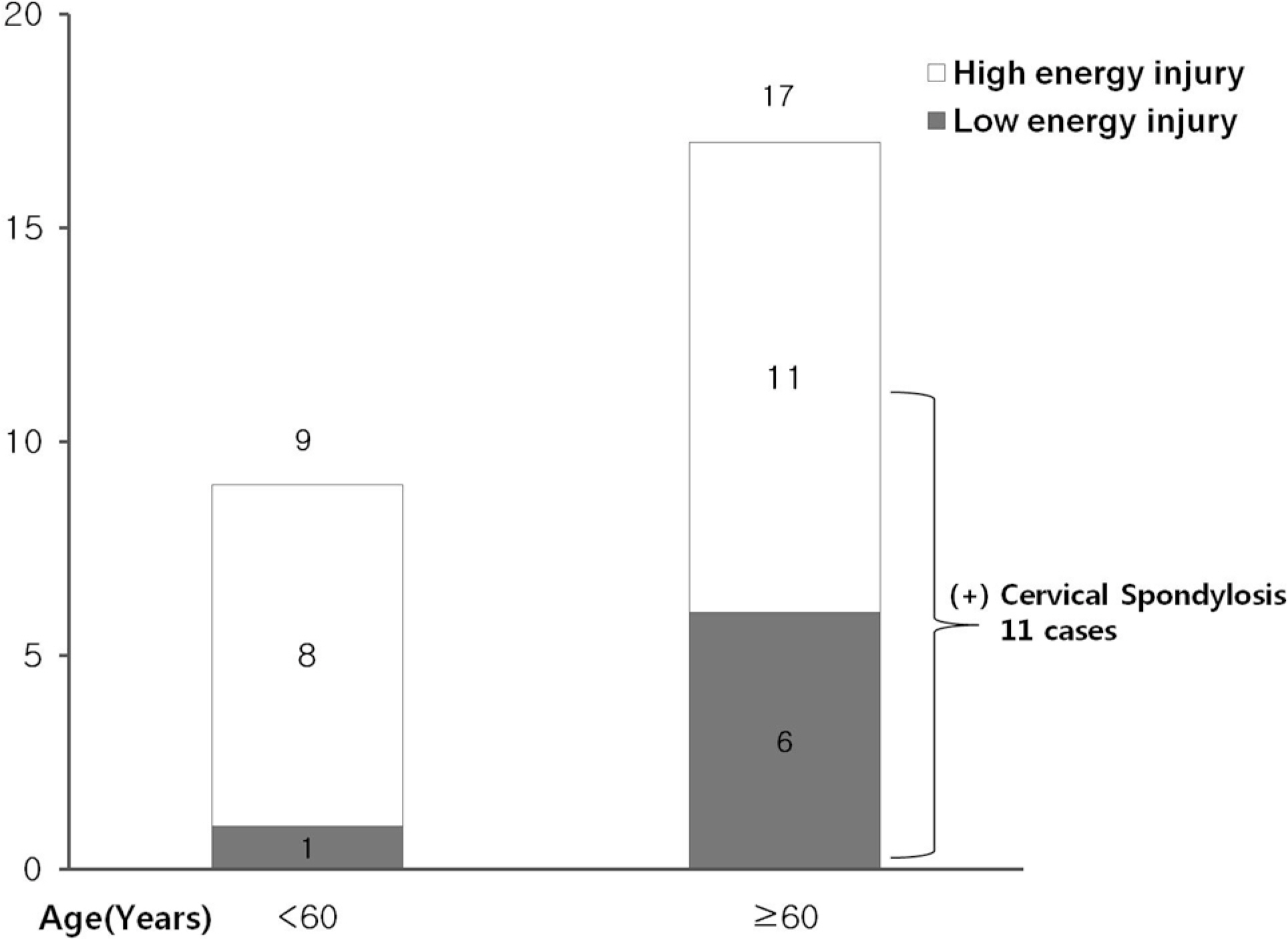
Fig 1. Relations between Age, Energy intensity of injury and the Presence of cervical spondylosis.
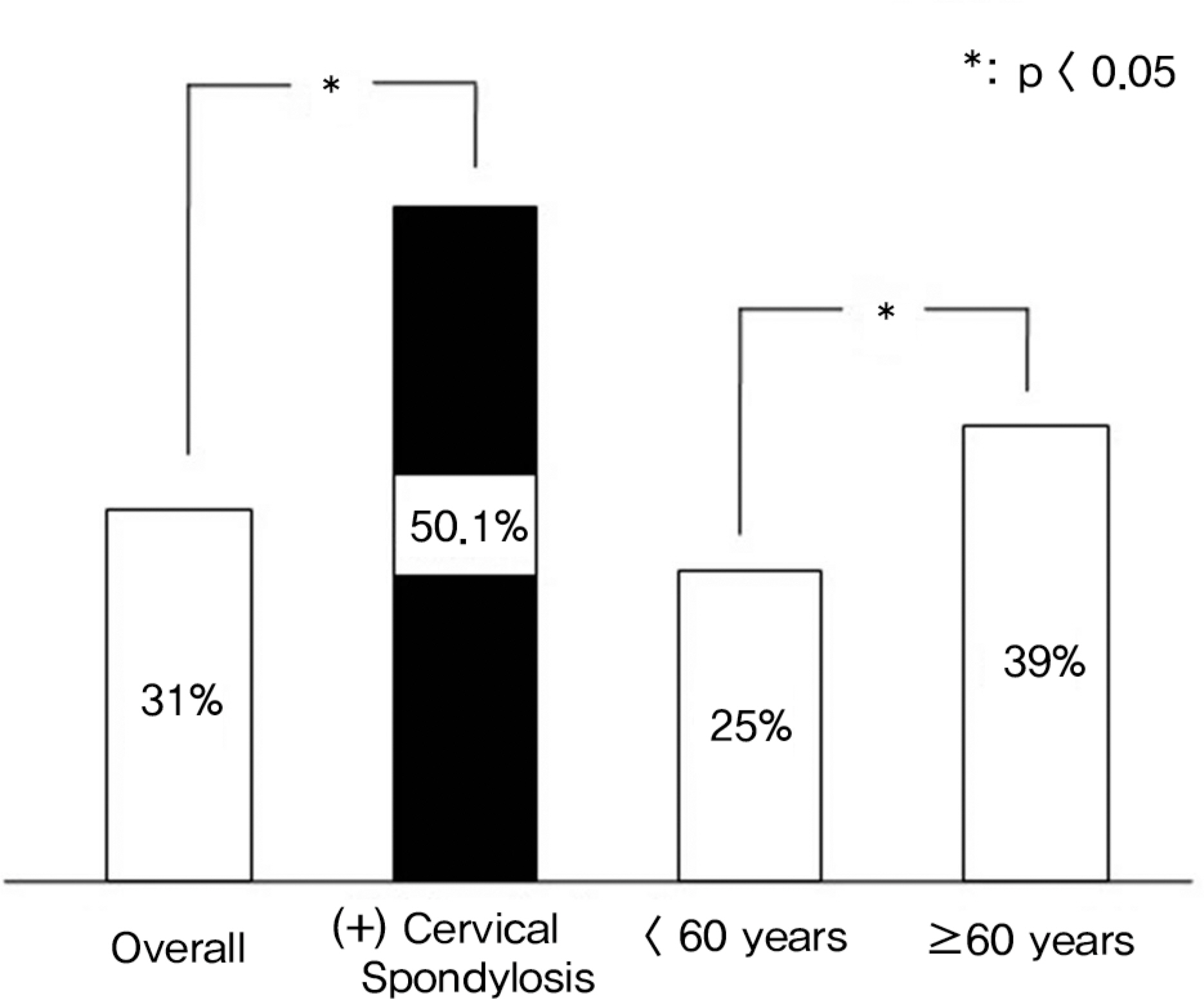
Fig 2. Postoperative neurological recovery rate.
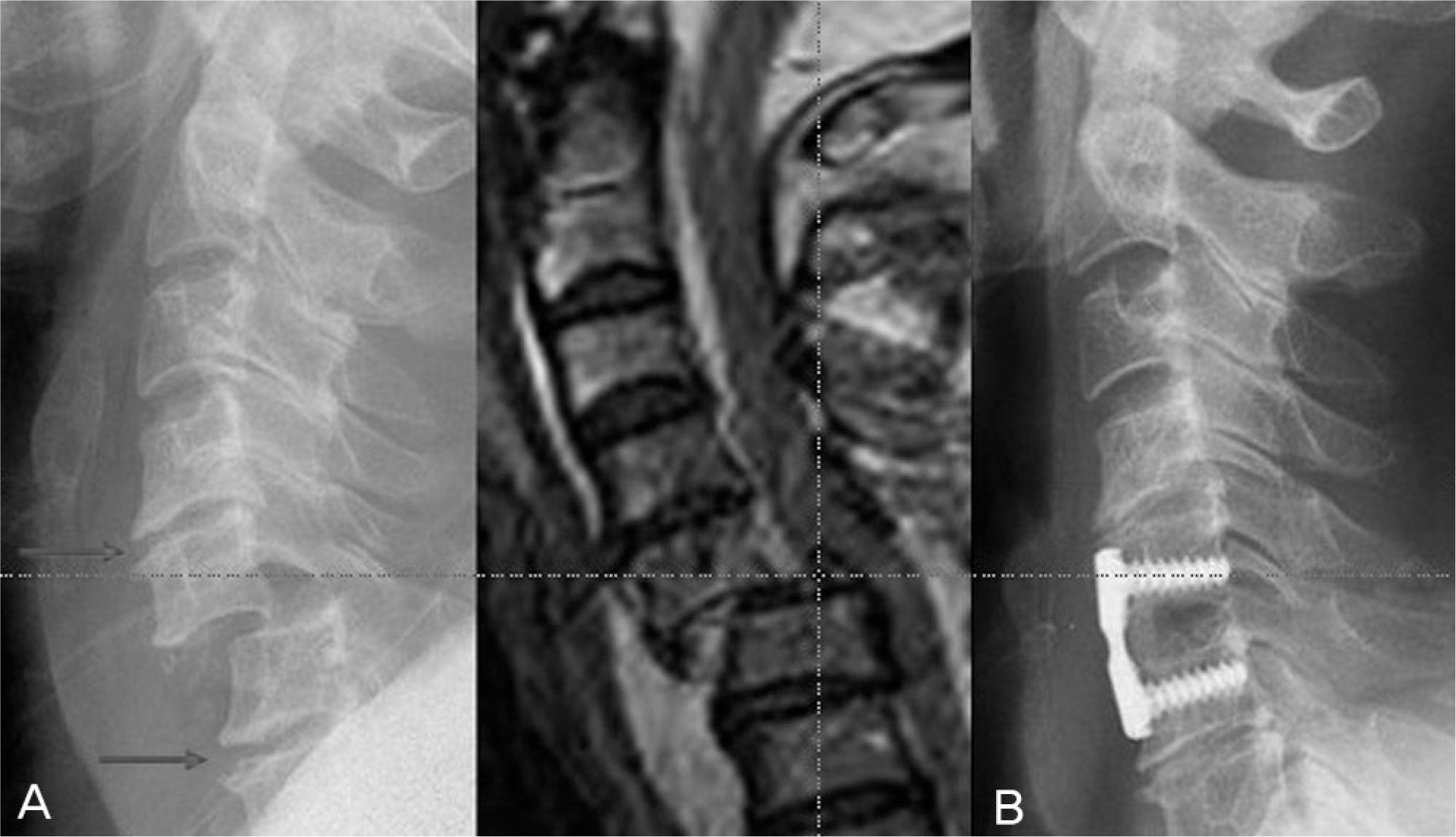
Fig 3. This 57 year old male patient with distractive-flexion injury(stage III) due to fall from 1.5m had incomplete cord injury. (A) Preoperative X-ray shows degenerative changes at adjacent segment of injured segment. (B) His neurological recovery rate of motor index score is 75% at the last follow-up.
Reference
-
1.Yang JY., Lee JK., Hong CH., Woo SM. Assessment of Quality of Life and Psychological Status in Spinal Cord Injury after Spinal Fracture. J Korean Soc Spine Surg. 2004. 11:285–90.
Article2.Kim YT., Lee CS., Lee SW., Choi DS., Lee SW. Prognostic Factors Affecting the Results of the Surgery for Cervical Spondylotic Myelopathy. J Korean Soc Spine Surg. 2005. 12:255–61.
Article3.Chung SS., Lee CS., Lee SG., Kim YH. Evaluation of Factors on Clinical Results Following Expansive Laminoplasty for Cervical Myelopathy. J Korean Orthop Assoc. 2000. 35:785–9.
Article4.Lee KY., Sohn SK., Lee MJ., Kim W. The Factors Affecting Surgical Results in Cervical Spondylotic Myelopathy. J Korean Spine Surg. 2005. 12:262–8.
Article5.Bohlman HH. Acute fracture and dislocation of the cervical spine. An analysis of three hundred hospitalized patients and review of the literature. J Bone Joint Surg Am. 1979. 61:1119–42.6.Jeong ST., Kim JS., Cho SH., Park HB. The Laminoplasty for Acute Cervical Spinal Cord Injury in Cervical Spondylosis. J Korean Orthop Assoc. 2005. 40:667–72.
Article7.Chung JY., Kim YS. Relationship between cervical cord injury and congenital spinal canal stenosis. J Korean Orthop Assoc. 1991. 26:1805–11.
Article8.Delamarter RB., Sherman JE., Carr JB. 1991 Volvo Award in experimental studies. Cauda equina syndrome: neurologic recovery following immediate, early, or late decompression. Spine. 1991. 16:1022–9.9.Delamarter RB., Sherman J., Carr JB. Pathophysiology of spinal cord injury. Recovery after immediate and delayed decompression. J Bone Joint Surg Am. 1995. 77:1042–9.
Article10.Ducker TB., Bellegarrigue R., Salcman M., Walleck C. Timing of operative care in cervical spinal cord injury. Spine. 1984. 9:525–31.
Article11.Ahn JS. Acute Spinal Cord Injury. J Korean Soc Spine Surg. 2000. 7:431–8.12.White AA., Southwick WO., Panjabi MM. Clinical instability in the lower cervical spine-a review of past and current concepts. Spine. 1976. 1:15–27.13.Jeong ST., Kim JS., Cho SH., Park HB. The Laminoplasty for Acute Cervical Spinal Cord Injury in Cervical Spondylosis. J Korean Orthop Assoc. 2005. 40:667–72.
Article14.Stauffer ES., Kelly EG. Fracture-dislocations of the cervical spine. Instability and recurrent deformity following treatment by anterior interbody fusion. J Bone Joint Surg Am. 1977. 59:45–8.
Article15.Song KJ., Lee KB. The Prognosis of the Acute Cervical Spinal Cord Injury. J Korean Orthop Assoc. 1998. 33:794–801.
Article16.Song KJ., Lee KB., Hwang BY., Lim YJ., Yoon JH. Relationship between Soft Tissue Damages and Spinal Cord Injury in Lower Cervical Spine Trauma. J Korean Orthop Assoc. 2005. 40:686–93.
Article17.Chung JY., Shin HC., Kim HS. Anterior Plate Fixation of the Fracture - Dislocation of Cervical Spine. J Korean Orthop Assoc. 1998. 6:1541–8.18.Frankel HL., Hancook DO., Hyslop G, et al. The value of postural reduction in the initial management of closed injuries of the spine with paraplegia and tetraplegia. I. Paraplegia. 1969. 7:179–92.19.Allen BL Jr., Ferguson RL., Lehmann TR., O'Brian RP. A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine. 1982. 7:1–27.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute Spinal Cord Injury after Cervical Nerve Root Block
- The Laminoplasty for Acute Cervical Spinal Cord Injury in Cervical Spondylosis
- Brown-Sequard Syndrome due to Herniated Cervical Disc
- Cervical Canal Size and Pressure in Experimental Spine Trauma
- Spinal Cord Injury by Ruptured Disc Particles in Cervical Spinal Trauma
