Two Cases of Unresectable Cholangiocarcinoma Treated by Yttrium-90 Microspheres
- Affiliations
-
- 1Department of Radiology, Korea University College of Medicine, Anam Hospital, Seoul, Korea. yhkku@kumc.or.kr
- 2Department of Gastroenterology, Korea University College of Medicine, Anam Hospital, Seoul, Korea.
- 3Department of Nuclear Medicine, Korea University College of Medicine, Anam Hospital, Seoul, Korea.
- KMID: 2208818
- DOI: http://doi.org/10.3348/jksr.2013.69.2.143
Abstract
- Intrahepatic cholangiocarcinoma (ICC) is a rare malignancy and many cases of ICCs are diagnosed in an unresectable state. Until now there has been no effective palliative treatment for these cases. Recently yttrium-90 (90Y) radioembolization has been highlighted as a new palliative treatment for these cases. In Korea, there has been no reported case of unresectable ICC which was treated by 90Y radioembolization up until now. We treated two cases of unresectable ICCs with 90Y radioembolization and the ICCs were necrotized effectively without significant toxicity.
MeSH Terms
Figure
-
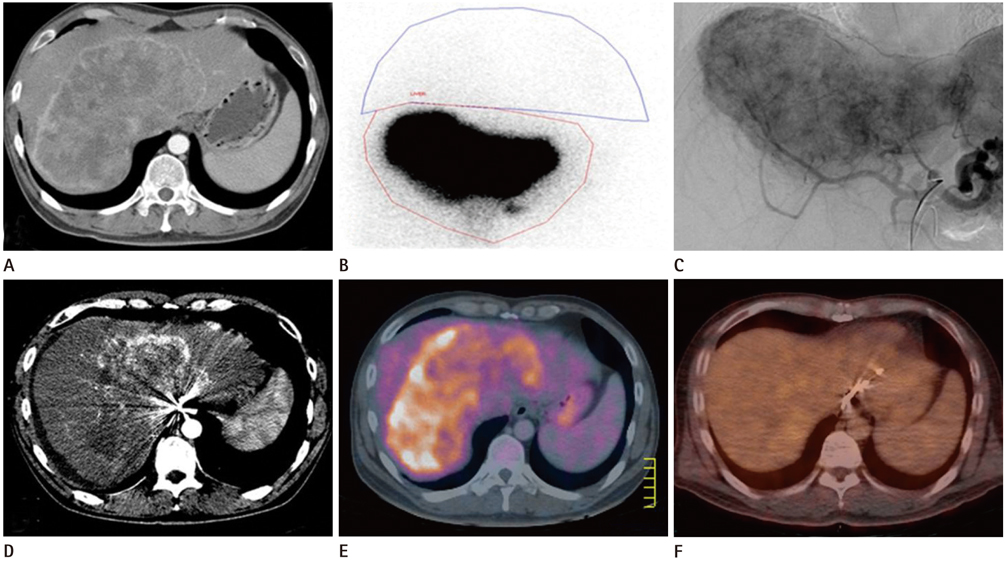
Fig. 1 A 38-year-old man with unresectable intrahepatic cholangiocarcinoma. A. Initial abdominal CT scan (arterial phase) shows 18 cm sized huge mass lesion with peripheral arterial enhancement in both hepatic lobes. B. Technetium 99m macroaggregated albumin scan shows low hepatopulmonary shunt rate (5.87%) and high tumor-to-normal ratio (7.89). C. Celiac arteriography shows hypervascular tumor in both hepatic lobes. D-F. At the 18-month after treatment, size of lesion is reduced (15 cm) and internal necrotic portion is increased. At the 18-month after treatment, previously noted hot-uptake lesion (E) is no more detected in positron emission tomography-CT scan (F).
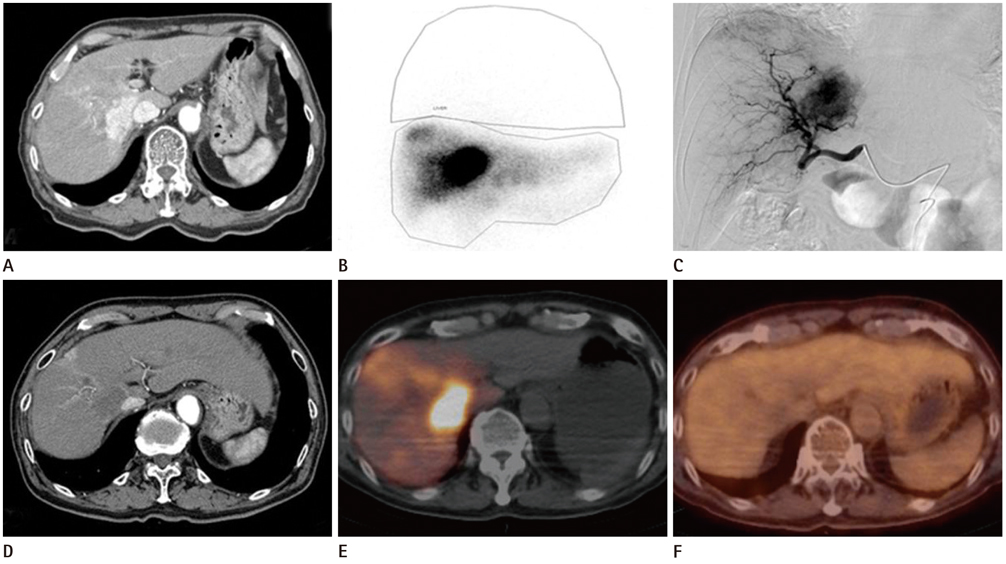
Fig. 2 A 74-year-old man with unresectable cholangiocarcinoma. A. Contrast enhanced CT scan at arterial phase shows 5.5 cm sized intrahepatic cholangiocarcinoma in S1, S7 and S8 before treatment. B. Technetium 99m macroaggregated albumin scan shows low hepatopulmonary shunt rate (4.12%) and high tumor-to-normal ratio (8.08). C. Celiac arteriography shows hypervascular tumor. D-F. At the 25-month after treatment, size of lesion is reduced (3.0 cm) and internal necrosis is noted. At the 25-month after treatment, previously noted hot-uptake lesion (E) is no more detected in positron emission tomography-CT scan (F).
Reference
-
1. Blechacz B, Gores GJ. Cholangiocarcinoma: advances in pathogenesis, diagnosis, and treatment. Hepatology. 2008; 48:308–321.2. Valle J, Wasan H, Palmer DH, Cunningham D, Anthoney A, Maraveyas A, et al. Cisplatin plus gemcitabine versus gemcitabine for biliary tract cancer. N Engl J Med. 2010; 362:1273–1281.3. Kiefer MV, Albert M, McNally M, Robertson M, Sun W, Fraker D, et al. Chemoembolization of intrahepatic cholangiocarcinoma with cisplatinum, doxorubicin, mitomycin C, ethiodol, and polyvinyl alcohol: a 2-center study. Cancer. 2011; 117:1498–1505.4. Vogl TJ, Naguib NN, Nour-Eldin NE, Bechstein WO, Zeuzem S, Trojan J, et al. Transarterial chemoembolization in the treatment of patients with unresectable cholangiocarcinoma: results and prognostic factors governing treatment success. Int J Cancer. 2012; 131:733–740.5. Park SY, Kim JH, Yoon HJ, Lee IS, Yoon HK, Kim KP. Transarterial chemoembolization versus supportive therapy in the palliative treatment of unresectable intrahepatic cholangiocarcinoma. Clin Radiol. 2011; 66:322–328.6. Kuhlmann JB, Euringer W, Spangenberg HC, Breidert M, Blum HE, Harder J, et al. Treatment of unresectable cholangiocarcinoma: conventional transarterial chemoembolization compared with drug eluting bead-transarterial chemoembolization and systemic chemotherapy. Eur J Gastroenterol Hepatol. 2012; 24:437–443.7. Kopek N, Holt MI, Hansen AT, Høyer M. Stereotactic body radiotherapy for unresectable cholangiocarcinoma. Radiother Oncol. 2010; 94:47–52.8. Murthy R, Nunez R, Szklaruk J, Erwin W, Madoff DC, Gupta S, et al. Yttrium-90 microsphere therapy for hepatic malignancy: devices, indications, technical considerations, and potential complications. Radiographics. 2005; 25:Suppl 1. S41–S55.9. Patel T. Increasing incidence and mortality of primary intrahepatic cholangiocarcinoma in the United States. Hepatology. 2001; 33:1353–1357.10. Shin HR, Oh JK, Lim MK, Shin A, Kong HJ, Jung KW, et al. Descriptive epidemiology of cholangiocarcinoma and clonorchiasis in Korea. J Korean Med Sci. 2010; 25:1011–1016.11. Ibrahim SM, Mulcahy MF, Lewandowski RJ, Sato KT, Ryu RK, Masterson EJ, et al. Treatment of unresectable cholangiocarcinoma using yttrium-90 microspheres: results from a pilot study. Cancer. 2008; 113:2119–2128.12. Saxena A, Bester L, Chua TC, Chu FC, Morris DL. Yttrium-90 radiotherapy for unresectable intrahepatic cholangiocarcinoma: a preliminary assessment of this novel treatment option. Ann Surg Oncol. 2010; 17:484–491.13. Hoffmann RT, Paprottka PM, Schön A, Bamberg F, Haug A, Dürr EM, et al. Transarterial hepatic yttrium-90 radioembolization in patients with unresectable intrahepatic cholangiocarcinoma: factors associated with prolonged survival. Cardiovasc Intervent Radiol. 2012; 35:105–116.14. Ho S, Lau WY, Leung TW, Chan M, Chan KW, Lee WY, et al. Tumour-to-normal uptake ratio of 90Y microspheres in hepatic cancer assessed with 99Tcm macroaggregated albumin. Br J Radiol. 1997; 70:823–828.15. van Persijn van Meerten EL, Gelderblom H, Bloem JL. RECIST revised: implications for the radiologist. A review article on the modified RECIST guideline. Eur Radiol. 2010; 20:1456–1467.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Radioembolization for hepatocellular carcinoma: what clinicians need to know
- Gastrectomy for the treatment of refractory gastric ulceration after radioembolization with 90Y microspheres
- Radioembolization for the Treatment of Primary and Metastatic Liver Cancers
- Radioembolization for the treatment of hepatocellular carcinoma
- Yttrium-90 Selective Internal Radiation Therapy with Glass Microspheres for Hepatocellular Carcinoma: Current and Updated Literature Review
