Validation of the KDRI in Korean Deceased Donor Kidney Transplantation
- Affiliations
-
- 1Division of Transplant and Vascular Surgery, Department of Surgery, Keimyung University Dongsan Medical Center, Keimyung University School of Medicine, Daegu, Korea. parkuijun@gmail.com
- KMID: 2202534
- DOI: http://doi.org/10.4285/jkstn.2014.28.2.78
Abstract
- BACKGROUND
The United Network for Organ Sharing developed the continuous kidney donor risk index (KDRI) for measurement of the spectrum of risk associated with the various factors known to influence graft failure. This study was conducted in order to validate the KDRI in assessment of deceased donor kidney in Koreans.
METHODS
Patients (n=404) who underwent kidney transplants performed at five transplantation centers from 2000 to 2010 were studied retrospectively. The distribution of the KDRI of donor kidneys was calculated and the distribution of kidney donors by standard criteria donor (SCD)/expanded criteria donor (ECD) and KDRI was compared. The KDRI were divided into five groups: <0.8, 0.8~1.0, 1.0~1.2, 1.2~1.4, and > or =1.4. Graft function and graft survival among KDRI groups were analyzed.
RESULTS
The mean KDRI was 1.01 (range, 0.55~1.88). More than 90% of donors had KDRI <1.4. The distribution of kidneys by KDRI groups was 22.8%, 32.7%, 27.5%, 9.9%, and 7.2%, respectively. Among kidneys with KDRI <0.8, 10.5% were ECD, whereas all of the kidneys with KDRI > or =1.4 were ECD. The estimated GFR at one-year in the KDRI groups was 72.2, 65.8, 63.2, 69.1, and 47.1 mg/dL, respectively. Graft function was significantly lower in those with KDRI > or =1.4 (P<0.001). Five-year graft survival in the KDRI groups was 91.6%, 92.2%, 91.3%, 94.1%, and 56.4%, respectively. Graft survival was also significantly lower in those with KDRI > or =1.4 (P=0.001).
CONCLUSIONS
The KDRI is a useful tool for estimation of posttransplant outcomes in the Korean population. The KDRI can be used by physicians as an additional assessment tool to assist in the decision making process regarding donor organ selection.
Keyword
MeSH Terms
Figure
-
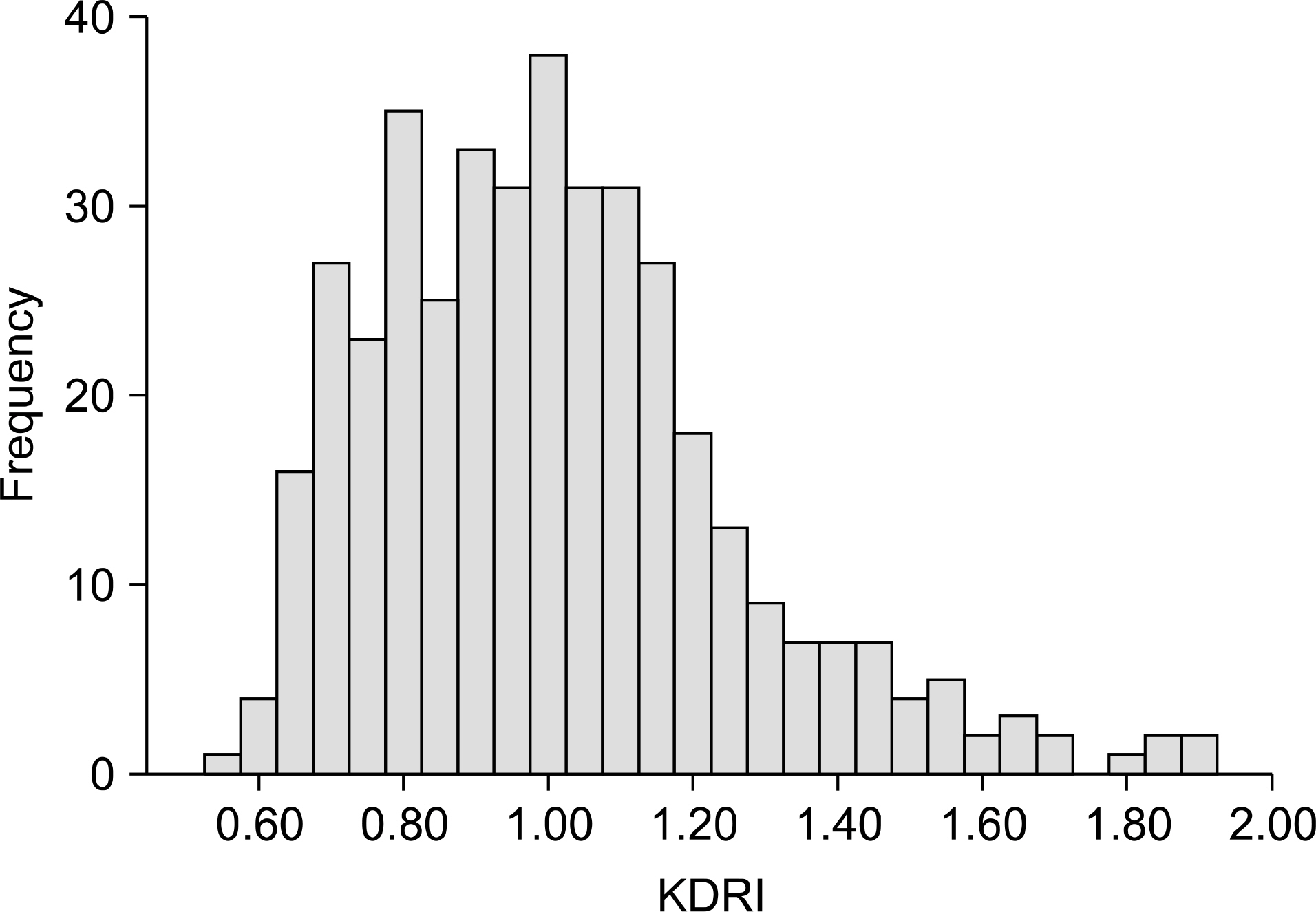
Fig. 1. Histogram of kidney donor risk index (KDRI). Fig. 3. Five-year graft survival by kidney donor risk index

Fig. 2. One year estimated glomerular filtration rate (GFR) by kidney donor risk index (KDRI) category.
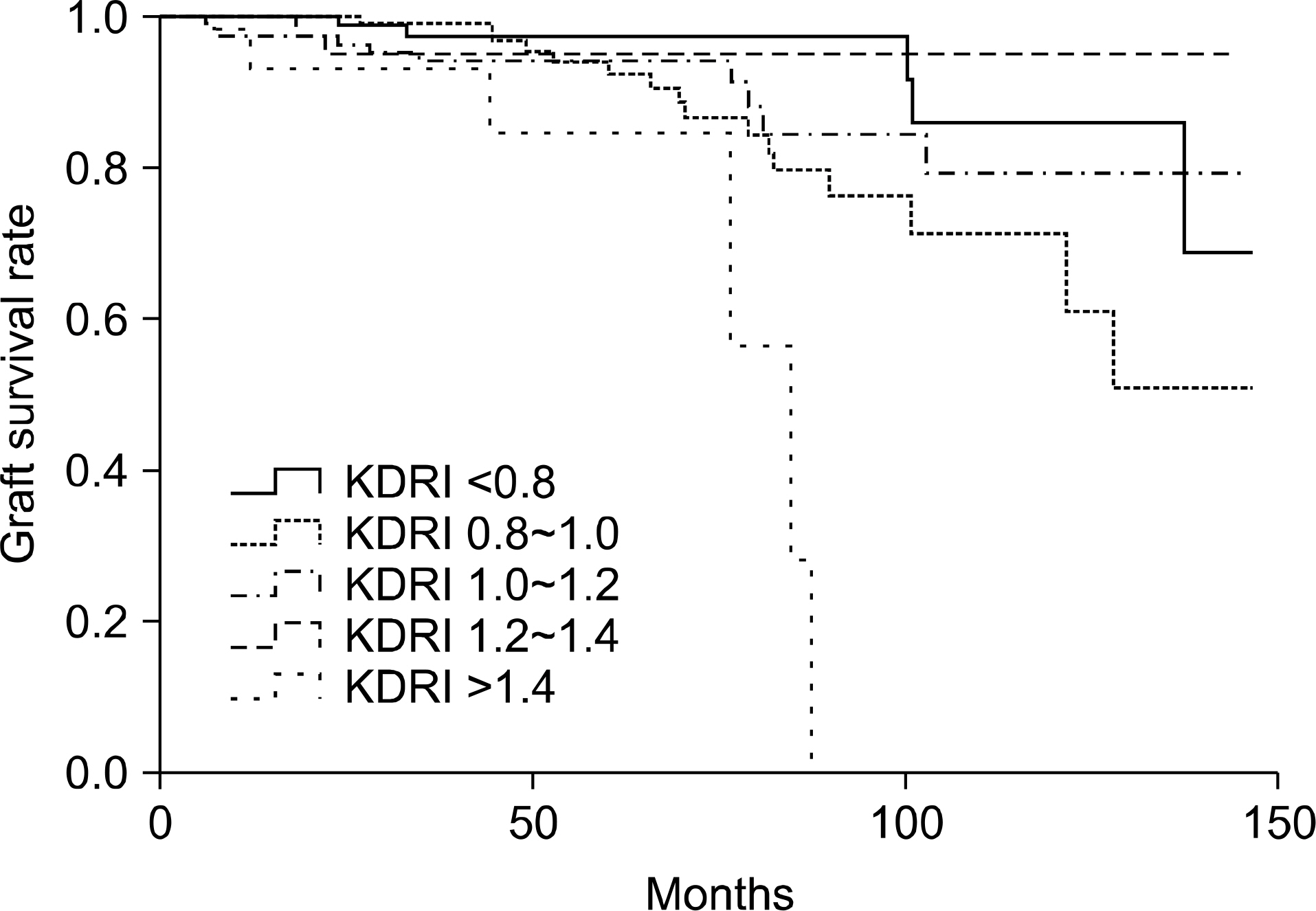
Fig. 3. Five-year graft survival by kidney donor risk index (KDRI) category.
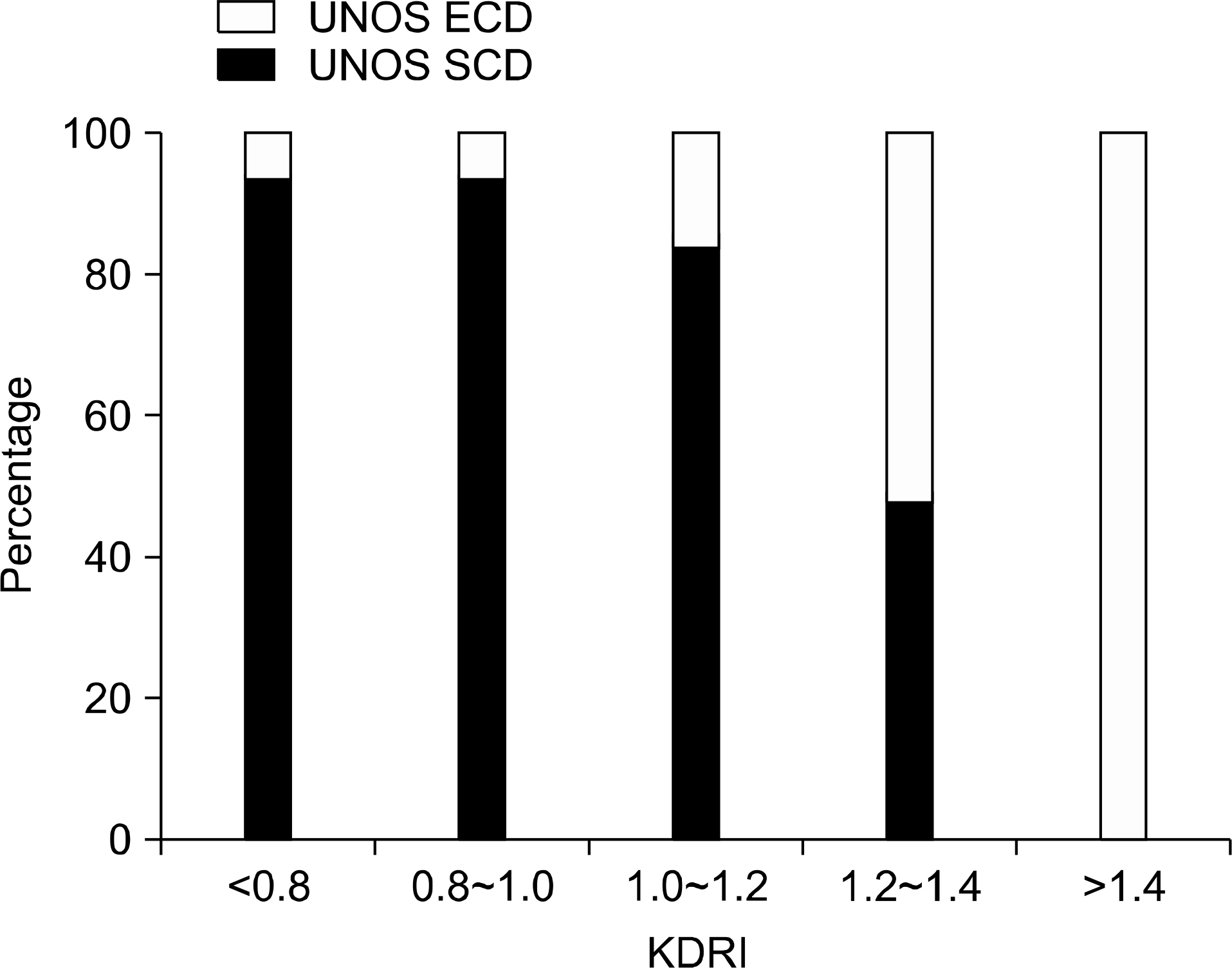
Fig. 4. Percentages of patients in expanded criteria donor (ECD) and standard criteria donor (SCD) by kidney donor risk index category. Abbreviation: UNOS, United Network for Organ Sharing.
Cited by 3 articles
-
Kidney Transplantation from Expanded Criteria Donor in Korea: It's Time to Have Our Own Criteria Based on Our Experiences
Shin-Seok Yang, Jae Berm Park
J Korean Soc Transplant. 2017;31(1):16-24. doi: 10.4285/jkstn.2017.31.1.16.Organ donation in Korea in 2018 and an introduction of the Korea national organ donation system
Won-Hyun Cho
Korean J Transplant. 2019;33(4):83-97. doi: 10.4285/jkstn.2019.33.4.83.Kidney Allocation: Present Status and Future Strategy
Yeong Hoon Kim
J Korean Soc Transplant. 2016;30(1):1-5. doi: 10.4285/jkstn.2016.30.1.1.
Reference
-
References
1). Korean Network for Organ Sharing. KONOS 2012 Annual Data Report [Internet]. Cheonwon: Korea Centers for Disease Control and Prevention;c2013. [cited 2014 Jan 14] Available from:. http://konos.go.kr.2). Crew RJ, Ratner LE. ABO-incompatible kidney transplantation: current practice and the decade ahead. Curr Opin Organ Transplant. 2010; 15:526–30.
Article3). Evenson AR. Utilization of kidneys from donation after circulatory determination of death. Curr Opin Organ Transplant. 2011; 16:385–9.
Article4). Schold JD, Segev DL. Increasing the pool of deceased donor organs for kidney transplantation. Nat Rev Nephrol. 2012; 8:325–31.
Article5). Rosengard BR, Feng S, Alfrey EJ, Zaroff JG, Emond JC, Henry ML, et al. Report of the Crystal City meeting to maximize the use of organs recovered from the cadaver donor. Am J Transplant. 2002; 2:701–11.
Article6). Rao PS, Schaubel DE, Guidinger MK, Andreoni KA, Wolfe RA, Merion RM, et al. A comprehensive risk quantification score for deceased donor kidneys: the kidney donor risk index. Transplantation. 2009; 88:231–6.
Article7). Health Resources and Services Administration. Organ Procurement and Transplantation Network (OPTN) [Internet]. Washington: Health Resources and Services Administration;c2013. [cited 2014 Jan 13]. Available from:. http://optn.transplant.hrsa.gov/resources.8). Jeong JC, Kim MG, Ro H, Kim YJ, Park HC, Kwon HY, et al. Kidney transplantation using expanded criteria donors in Korea. Transplant Proc. 2012; 44:54–6.
Article9). Kim JM, Kim SJ, Joh JW, Kwon CH, Song S, Shin M, et al. Is it safe to use a kidney from an expanded criteria donor? Transplant Proc. 2011; 43:2359–62.
Article10). Gourishankar S, Grebe SO, Mueller TF. Prediction of kidney graft failure using clinical scoring tools. Clin Transplant. 2013; 27:517–22.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Evaluation and Utilization of Expanded Criteria Dornor
- A Preliminary Study to Revise the Marginal Donor Criteria of KONOS in Deceased Donor Kidney Transplantation
- Current Status of Deceased Donor Organ Recovery and Sharing in Korea
- Factors affecting discard of deceased donor kidneys of Korea
- Thrombotic microangiopathy, rare cause of deceased donor acute kidney injury: is a donor biopsy necessary before donation?
