Trigger Wrist
- Affiliations
-
- 1Department of Orthopaedic Surgery, Kyung Hee University Hospital at Gangdong, Seoul, Korea. ljhos69@naver.com
- 2Department of Orthopaedic Surgery, Kyung Hee University Hospital, Seoul, Korea.
- 3Department of Pathology, Kyung Hee University Hospital at Gangdong, Seoul, Korea.
- KMID: 2194160
- DOI: http://doi.org/10.12790/jkssh.2013.18.2.71
Abstract
- Triggering at the wrist during active flexion and extension of the fingers or wrists is very rare. It is caused by tumors, inflammation, and anomalous muscle belly. We report two cases of trigger wrist caused by synovial hypertrophy and fibroma of flexor tendon.
Keyword
Figure
-

Fig. 1. (A) Sagittal T2 magnetic resonance images shows nodular mass (arrows) surrounded by the flexor tendons at the just distal level to the transverse carpal ligament. The mass shows heterogeneously increased signal intensity on T2-weighted image. (B) On the contrast enhanced axial image, the lesion shows eccentric nodular and peripheral enhancement within the mass (arrows). Flattening and weak enhancement of the median nerve suggest entrapment neuropathy (arrowhead).

Fig. 2. (A) Irregularly shaped nodular and streaky portion of the mass was freely separated from the tendon. However the proximal end of the mass was fixed to the tendon at the level of proximal entry of carpal tunnel. (B) A photograph taken just after the mass removal. There was no noticeable abnormality of tendon or tendon sheath. Note the separate sheath that encapsulated the mass. (C) A photograph of the mass.
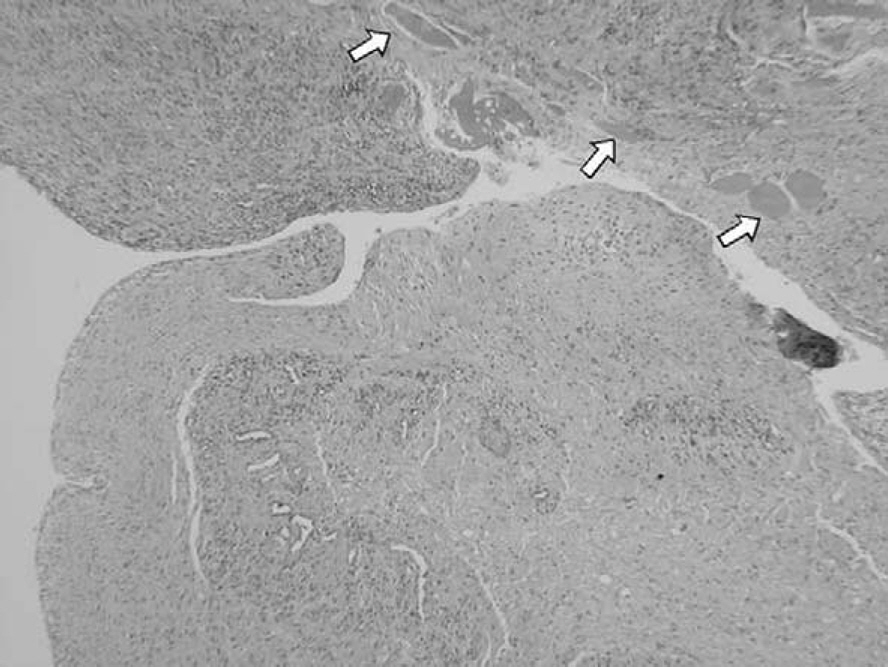
Fig. 3. A picture of low power microscopic examination (×100) with H&E staining shows portions of muscle bellies (arrows) and surrounding synovial, capillary and fibrous overgrowth. There is no inflammatory cell infiltration except scanty macrophages.
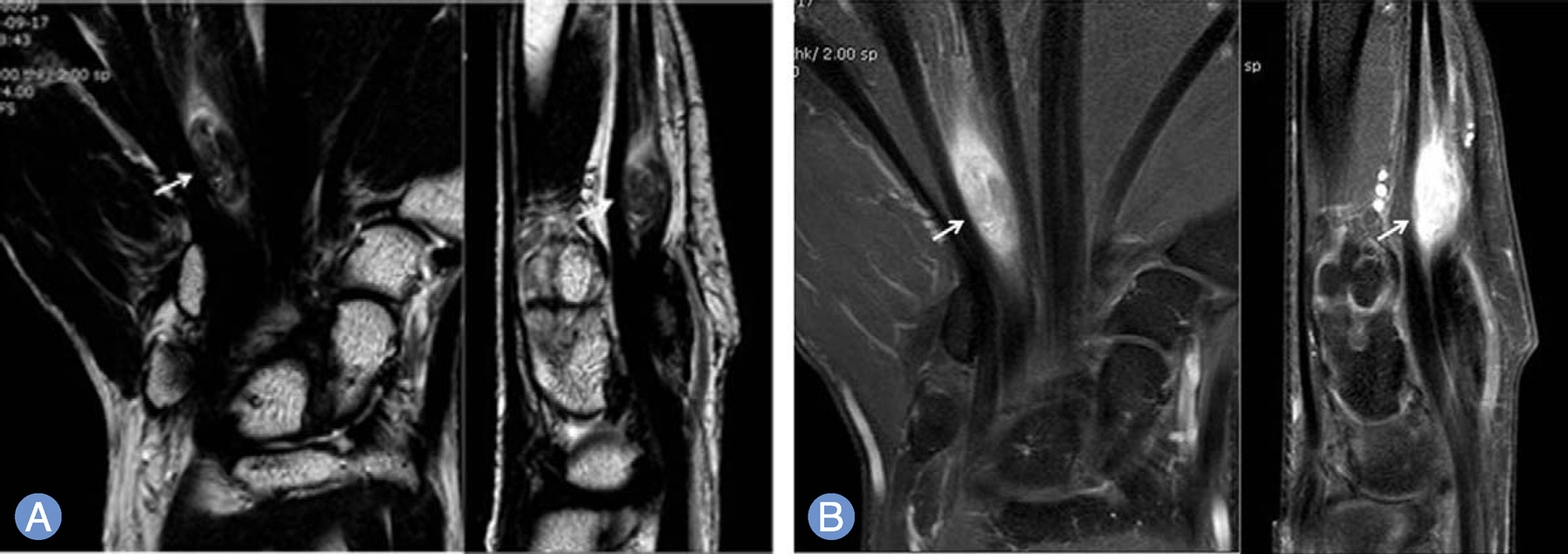
Fig. 4. (A) T2-weighted magnetic resonance images show well-defined oval mass (arrows) with low heteogenous signal intensity between flexor tendon underneath transverse carpal ligament. (B) Enhanced images show heterogenous enhance-
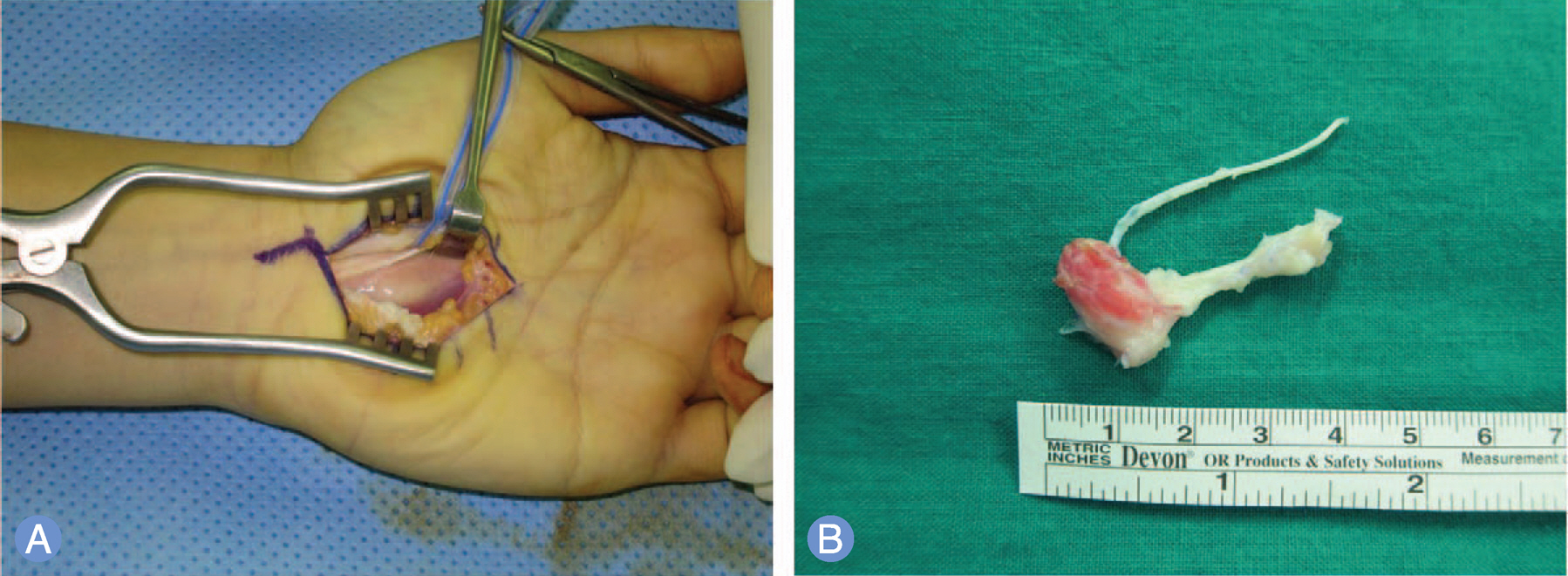
Fig. 5. (A) Round gray mass was identified underneath transverse carpal ligament, which was originated from flexor digitorum profundus and connected lumbrical muscle. (B) Excised mass, measuring 2×2×1 cm.
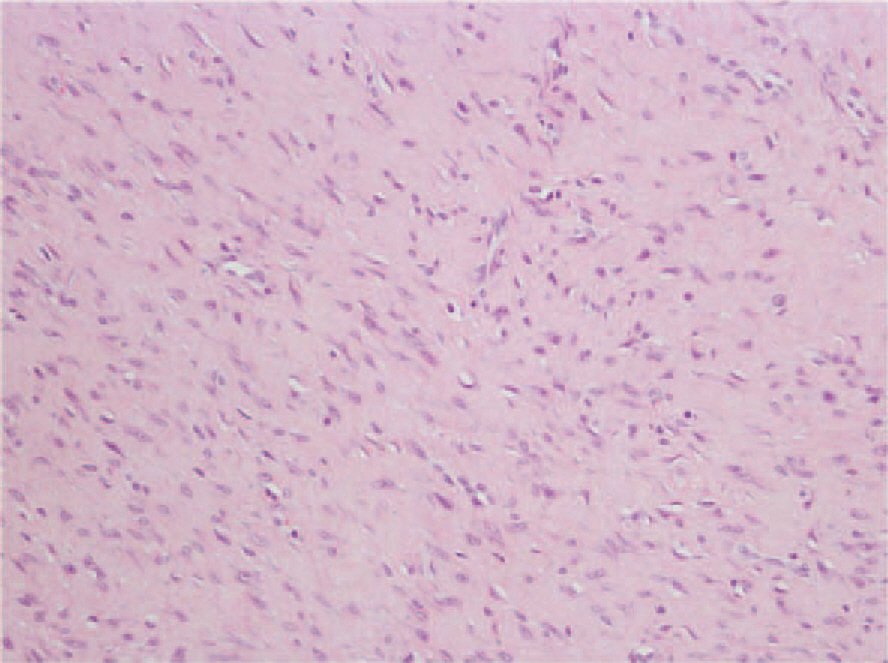
Fig. 6. Microscopic examination (×200) with H&E staining shows mainly spindle-shaped cell intermixed with collagen fibers and there are no multinucleated giant cells, xanthoma cells, or hemosiderin deposits observed.
Reference
-
1. Parmaksizoglu F, Beyzadeoglu T, Yildirim S. Haemangioma originating from a tendon sheath as an unusual cause of trigger wrist: case report. Handchir Mikrochir Plast Chir. 2003; 35:64–5.
Article2. Smith RD, O'Leary ST, McCullough CJ. Trigger wrist and flexor tenosynovitis. J Hand Surg Br. 1998; 23:813–4.
Article3. Sonoda H, Takasita M, Taira H, Higashi T, Tsumura H. Carpal tunnel syndrome and trigger wrist caused by a lipoma arising from flexor tenosynovium: a case report. J Hand Surg Am. 2002; 27:1056–8.
Article4. Suematsu N, Hirayama T, Takemitsu Y. Trigger wrist caused by a giant cell tumour of tendon sheath. J Hand Surg Br. 1985; 10:121–3.
Article5. Pople IK. Trigger wrist due to idiopathic synovial hypertrophy. J Hand Surg Br. 1986; 11:453–4.
Article6. Lemon RA, Engber WD. Trigger wrist: a case report. J Hand Surg Am. 1985; 10:61–3.
Article7. Yamazaki H, Uchiyama S, Kato H. Snapping wrist caused by tenosynovitis of the extensor carpi radialis longus tendon subsequent to subcutaneous muscle rupture in the forearm: case report. J Hand Surg Am. 2010; 35:1964–7.
Article8. Desai SS, Pearlman HS, Patel MR. Clicking at the wrist due to fibroma in an anomalous lumbrical muscle: a case report and review of literature. J Hand Surg Am. 1986; 11:512–4.
Article9. Kernohan JG, Benjamin A, Simpson D. Trigger wrist due to anomalous flexor digitorum profundus muscle in association with fibroma of tendon sheath. Hand. 1982; 14:59–60.
Article10. Jackson WT, Protas JM. Snapping scapholunate subluxation. J Hand Surg Am. 1981; 6:590–4.
Article11. Zachee B, DeSmet L, Fabry G. A snapping wrist due to a loose body. Arthroscopic diagnosis and treatment. Arthroscopy. 1993; 9:117–8.
Article12. Weeks PM, Young VL, Gilula LA. A cause of painful clicking wrist: a case report. J Hand Surg Am. 1979; 4:522–5.
Article13. Eibel P. Trigger Wrist with Intermittent Carpal Tunnel Syndrome: A Hitherto Undescribed Entity with Report of a Case. Can Med Assoc J. 1961; 84:602–5.14. Carvell JE, Mowat AG, Fuller DJ. Trigger wrist phenomenon in rheumatoid arthritis. Hand. 1983; 15:77–81.
Article15. Minami A, Ogino T. Trigger wrist caused by a partial laceration of the flexor superficialis tendon of the ring finger. J Hand Surg Br. 1986; 11:457–9.
Article16. Eckhardt WA, Palmer AK. Recurrent dislocation of extensor carpi ulnaris tendon. J Hand Surg Am. 1981; 6:629–31.
Article17. Giannikas D, Karabasi A, Dimakopoulos P. Trigger wrist. J Hand Surg Eur Vol. 2007; 32:214–6.
Article18. Kellgren JH, Ball J. Tendon Lesions in Rheumatoid Arthritis. Ann Rheum Dis. 1950; 9:48–65.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Trigger Wrist
- "Trigger Finger at the Wrist" due to Anomalous Flexor Digitorum Superficialis Muscle Belly with Carpal Tunnel Syndrome: A Case Report
- Trigger Wrist and Carpal Tunnel Syndrome Caused by a Fibroma of the Flexor Tendon
- Total Wrist Arthroplasty (Three Cases Report)
- The Wrist Arthroscopy in Diagnosis and Treatment of wrist pain patients
