Surgical Management of Pisiform Bone Deformity Associated with Tendonitis of Flexor Carpi Ulnaris
- Affiliations
-
- 1Department of Orthopedics, Yonsei University Wonju College of Medicine, Wonju, Korea. jroh@yonsei.ac.kr
- KMID: 2194143
- DOI: http://doi.org/10.12790/jkssh.2013.18.3.132
Abstract
- PURPOSE
This study was performed to investigate the degree of symptom improvement after removal of bone fragment in patients with deformed pisiform bone associated with tendonitis of flexor carpi ulnaris.
METHODS
Pisiform bone fragment removal was performed in 12 patients who had failed conservative treatment from January 2008 to December 2011. They were followed up at 2 weeks, 1 month, 2 months, 6 months, and 12 months after surgery. Their symptoms were assessed with Green score.
RESULTS
Eleven of 12 patients who underwent bone fragment removal showed symptom improvement. Symptoms worsened in 1 patient due to pain and restricted range of motion caused by postoperative scar.
CONCLUSION
The results of this study suggest that removal of bone fragment may be an effective treatment in patients with tendonitis of flexor carpi ulnaris accompanied by pisiform bone deformity whose pain does not improve with conservative management.
Figure
-

Fig. 1. Bone widening of the pisiform bone in carpal tunnel X-ray view of the patient with tendonitis of flexor carpi ulnaris caused by repeated movement and inflammation.
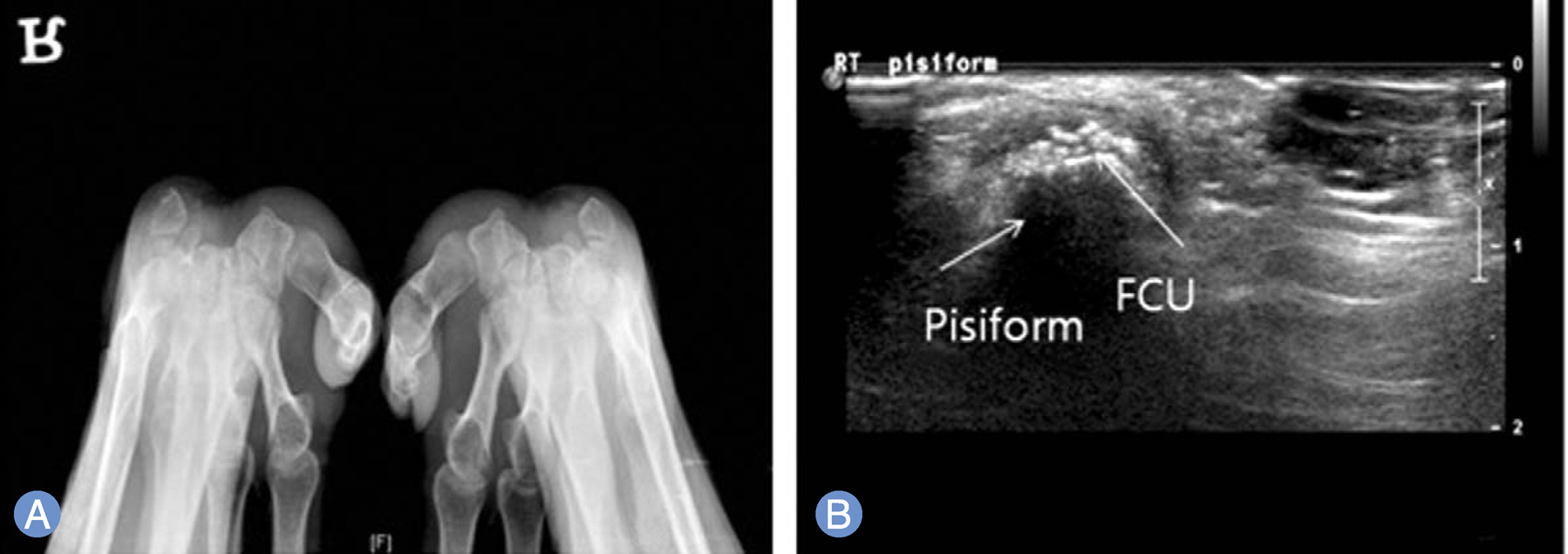
Fig. 2. Radiograph and ultrasonograph of the patient with tendonitis of flexor carpi ulnaris. (A) Bone widening of the pisiform bone can be observed on radiograph. (B) Ultrasonograph also shows calcified tissues between the pisiform bone and flexor carpi ulnaris (FCU).
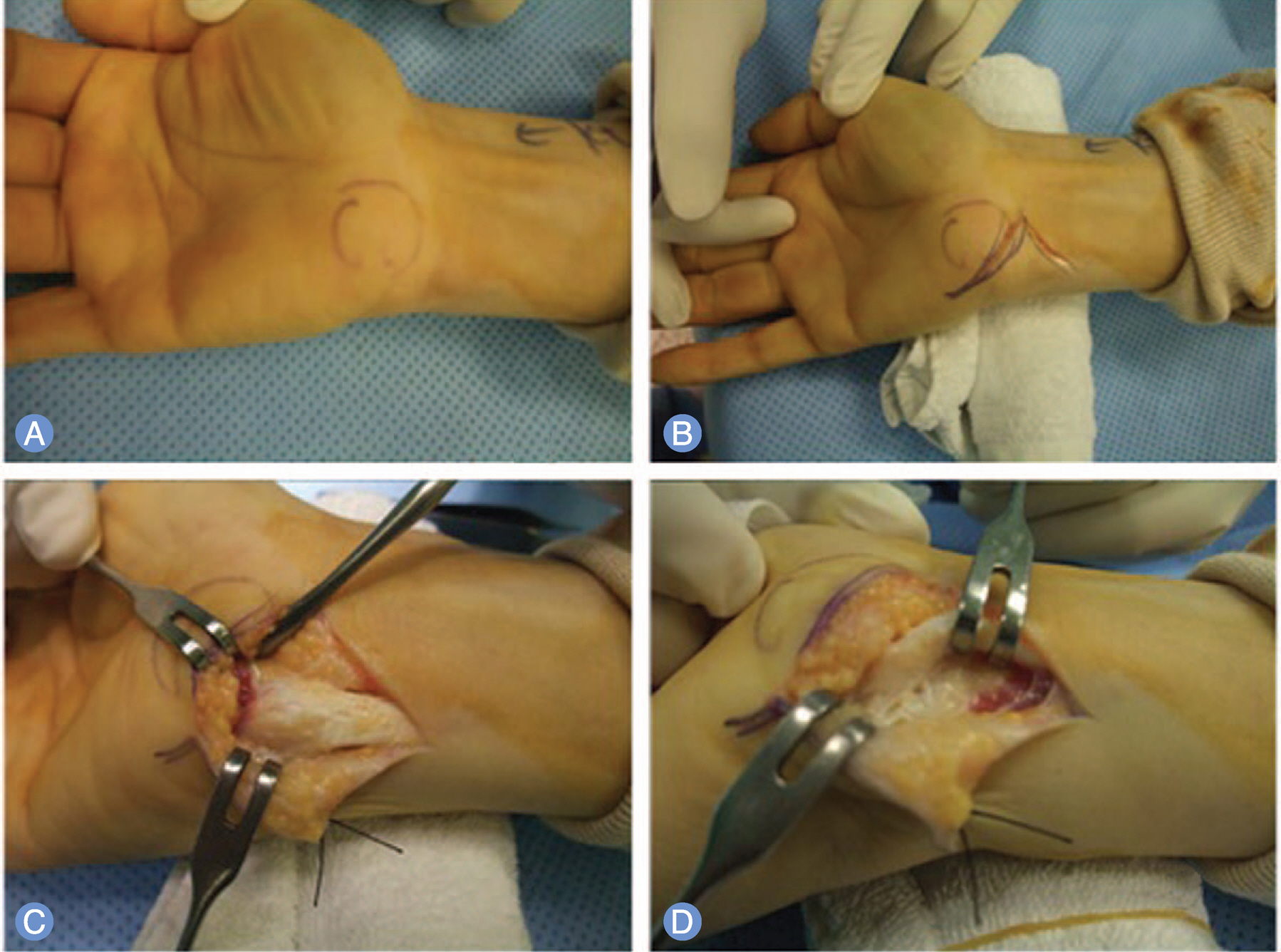
Fig. 3. Surgical technique on bone widening due to inflammation of the flexor carpi ulnaris. (A) The pisiform bone at the ulnar side of the palm was checked through palpation. (B) A V-shaped skin incision was made at the ulnar side to confirm the location of the pisiform bone. (C) The skin was retracted to obtain operative window, and the flexor carpi ulnaris was found after dissection of the soft tissue and the fascia. (D) The flexor carpi ulnaris was retract towards the radial side to expose the pisiform bone.
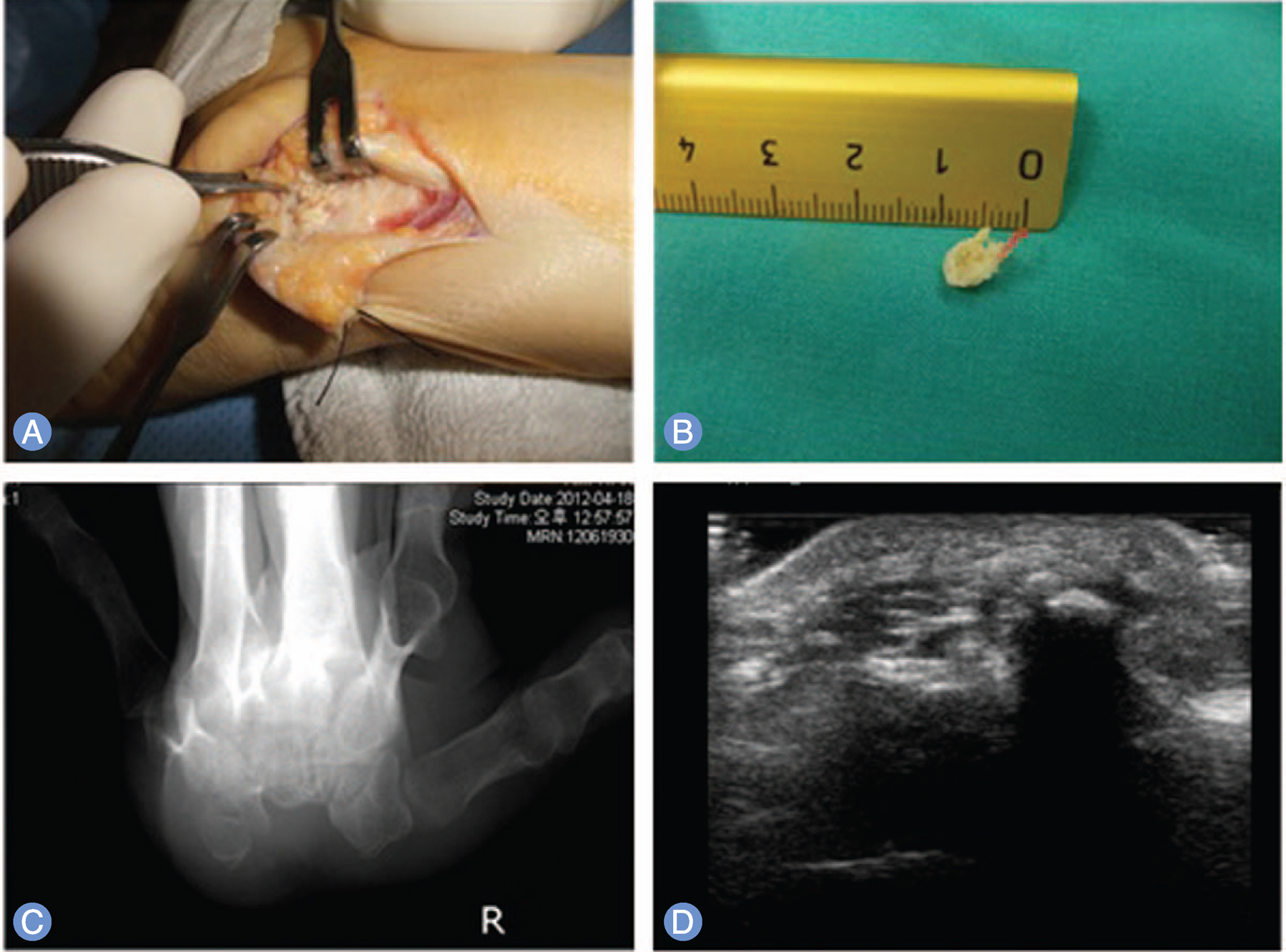
Fig. 4. Surgical technique on bone widening due to inflammation of the flexor carpi ulnaris. (A) The hypertrophied portion of the pisiform bone found after radial retraction of the flexor carpis ulnaris is marked and is resected. (D) Bone fragment after removal. (C) Carpal tunnel X-ray after bone fragment removal. (D) Bone fragments observed preoperative are not present.
Reference
-
1. Shin AY, Deitch MA, Sachar K, Boyer MI. Ulnar-sided wrist pain: diagnosis and treatment. Instr Course Lect. 2005; 54:115–28.2. Dilley DF, Tonkin MA. Acute calcific tendinitis in the hand and wrist. J Hand Surg Br. 1991; 16:215–6.
Article3. Gandee RW, Harrison RB, Dee PM. Peritendinitis calcarea of flexor carpi ulnaris. AJR Am J Roentgenol. 1979; 133:1139–41.
Article4. Martin JF, Brogdon BG. Peritendinitis calcarea of the hand and wrist. Am J Roentgenol Radium Ther Nucl Med. 1957; 78:74–85.5. Moyer RA, Bush DC, Harrington TM. Acute calcific tendinitis of the hand and wrist: a report of 12 cases and a review of the literature. J Rheumatol. 1989; 16:198–202.6. Eshed I, Feist E, Althoff CE, et al. Tenosynovitis of the flexor tendons of the hand detected by MRI: an early indicator of rheumatoid arthritis. Rheumatology (Oxford). 2009; 48:887–91.
Article7. Maffulli N, Denaro V, Loppini M. Haglund's deformity. Foot Ankle Int. 2012; 33:807–8.8. Kang S, Thordarson DB, Charlton TP. Insertional Achilles tendinitis and Haglund's deformity. Foot Ankle Int. 2012; 33:487–91.
Article9. Jung HG, Carag JA, Park JY, Bae EJ, Lim SD, Kim HS. Osteochondroma of the calcaneus presenting as Haglund's deformity. Foot Ankle Surg. 2011; 17:e20–2.
Article10. Peterson KS, Jedlicka NM, Vardaxis VG, Yoho RM. Radiographic analysis of Haglund's deformity: an evaluation of NCSP and RCSP. J Am Podiatr Med Assoc. 2010; 100:78–9.
Article11. Palmieri TJ. Pisiform area pain treatment by pisiform excision. J Hand Surg Am. 1982; 7:477–80.12. Fischer E. Piso-triquetral arthrosis and the so-called pisiform secundarium. Radiologe. 1988; 28:338–44.13. Backhaus M. Ultrasound and structural changes in inflammatory arthritis: synovitis and tenosynovitis. Ann N Y Acad Sci. 2009; 1154:139–51.14. D'Agostino MA, Conaghan PG, Naredo E, et al. The OMERACT ultrasound task force: advances and priorities. J Rheumatol. 2009; 36:1829–32.15. Cooney WP 3rd. Bursitis and tendinitis in the hand, wrist, and elbow. An approach to treatment. Minn Med. 1983; 66:491–4.16. Leadbetter WB, Mooar PA, Lane GJ, Lee SJ. The surgical treatment of tendinitis. Clinical rationale and biologic basis. Clin Sports Med. 1992; 11:679–712.
Article17. Pierre A, Le Nen D, Hu W, Dubrana F, Saraux A, Chaise F. Treatment of piso-triquetral pain by excision of the pisiform: report of fifteen cases. Chir Main. 2003; 22:37–42.18. Iagnocco A, Filippucci E, Perella C, et al. Clinical and ultrasonographic monitoring of response to adalimumab treatment in rheumatoid arthritis. J Rheumatol. 2008; 35:35–40.19. Schueller-Weidekamm C, Schueller G, Aringer M, Weber M, Kainberger F. Impact of sonography in gouty arthritis: comparison with conventional radiography, clinical examination, and laboratory findings. Eur J Radiol. 2007; 62:437–43.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Treatment of Chronic Flexor Carpi Ulnaris Tendinopathy
- Tendon Problems of the Ulnar Wrist
- Accessory muscle in the forearm: a clinical and embryological approach
- Ulnar nerve Compression Syndrome due to anomalous Branch of the Ulnar Nerve Piercing the Flexor Carpi Ulnaris: Report of one case
- Tendonitis of the Flexor Hallucis Longus with Triggering of the Great Toe: A Case Report
