Rapid Visual Deterioration Caused by Posterior Fossa Arachnoid Cyst
- Affiliations
-
- 1Department of Neurosurgery, Sungkyunkwan University, School of Medicine, Kangbuk Samsung Hospital, Seoul, Korea. kkimsion@hanmail.net
- 2Department of Radiology, Sungkyunkwan University, School of Medicine, Kangbuk Samsung Hospital, Seoul, Korea.
- 3Graduate School of Medicine, Yonsei University, Seoul, Korea.
- KMID: 2192114
- DOI: http://doi.org/10.3340/jkns.2016.59.3.314
Abstract
- Posterior fossa is a site next to the middle fossa where arachnoid cyst frequently occurs. Generally, most arachnoid cysts are asymptomatic and are found incidentally in most cases. Although arachnoid cysts are benign and asymptomatic lesions, patients with posterior fossa arachnoid cysts often complain of headaches, gait disturbance, and ataxia due to the local mass effects on the cerebellum. We observed a patient with a posterior fossa arachnoid cyst who had visual symptoms and a headache, but did not have gait disturbance and ataxia. We recommended an emergency operation for decompression, but the patient refused for personal reasons. After 7 days, the patient revisited our hospital in a state of near-blindness. We suspected that the arachnoid cyst induced the hydrocephalus and thereby the enlarged third ventricle directly compressed optic nerves. Compressed optic nerves were rapidly aggravated during the critical seven days; consequently, the patient's vision was damaged despite the operation. Considering the results of our case, it is important to keep in mind that the aggravation of symptoms cannot be predicted; therefore, symptomatic arachnoid cysts should be treated without undue delay.
MeSH Terms
Figure
-
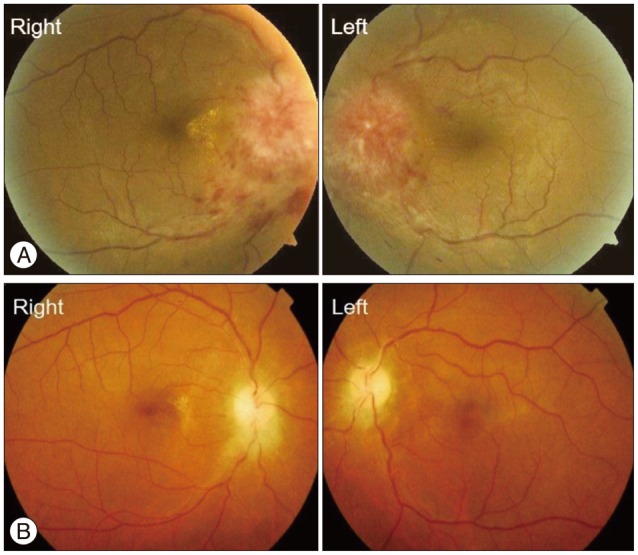
Fig. 1 Fundoscopy. A : One week before the operation. B : Five months after the operation.
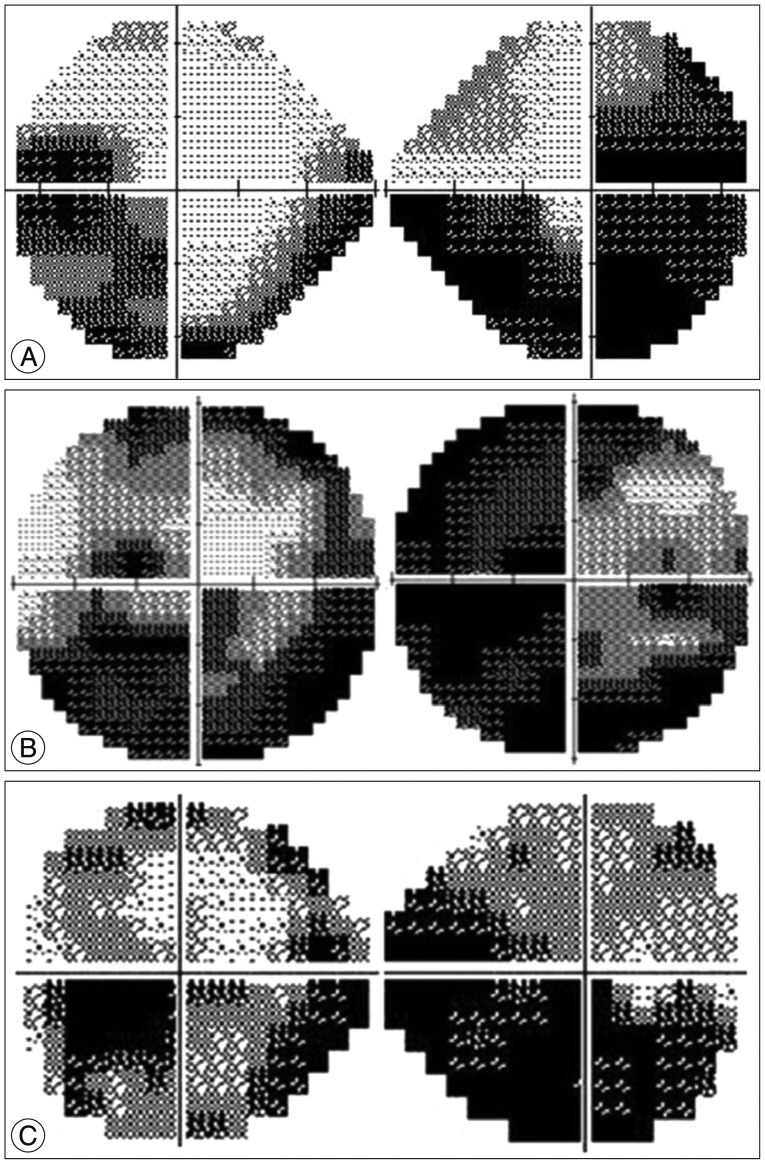
Fig. 2 Visual field test. A : One week before the operation. B : Operation date. C : Five months after operation.
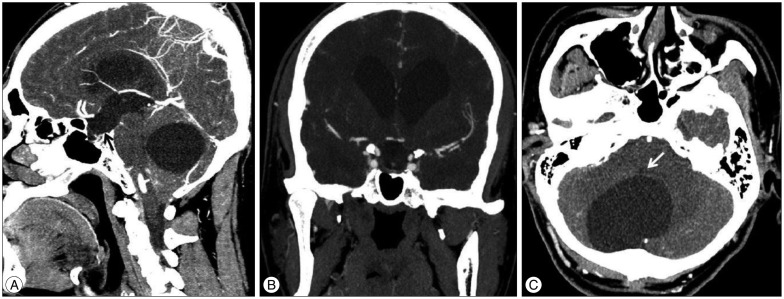
Fig. 3 Preoperative enhanced CT scans. A : Sagittal cutting image on the midline. Black arrow : the enlarged third ventricle is compressing the optic chiasm and sella turcica. B : Coronal cutting image on the optic chiasm. Pituitary gland is compressed by the third ventricle and sella turcica is filled with the cerebrospinal fluid. C : Axial cutting image on the cerebellar level. White arrow : a large arachnoid cyst is compressing the fourth ventricle and circumferential cerebellum.
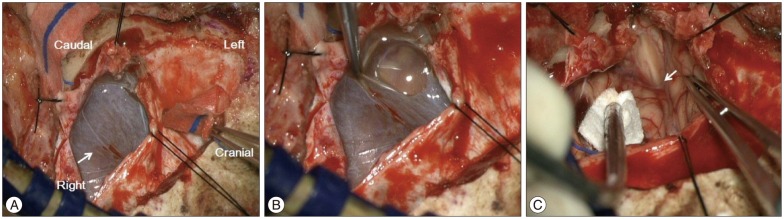
Fig. 4 Intraoperative microscopic images. A : After the dual incision, thin arachnoid membrane (white arrow) is found that is covers the arachnoid cyst. B : Clear fluid slopped over the arachnoid membranes. C : White arrow : after an excision of the arachnoid membrane, the cerebrospinal fluid flows through foramen of magendie are observed.

Fig. 5 The collapsed cystic membrane was stained by hematoxylin and eosin (H&E) stain. Under the high power field microscopy, requested membrane was composed by fibrocollagenous tissues and thin cuboidal lining cells were attached to the membrane. Atypical cell and abnormal mitosis was not found (outlet figure : H&E, ×4; inlet figure : H&E, ×20).
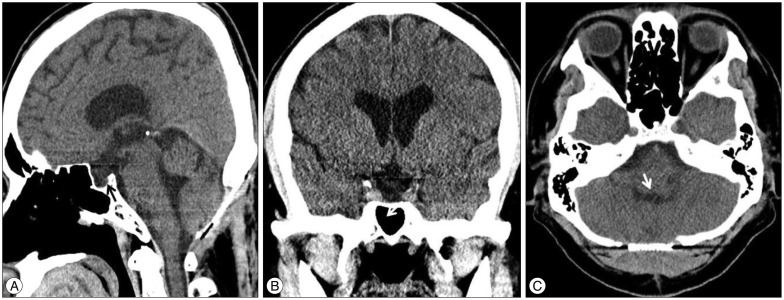
Fig. 6 Five months after operation. A : Sagittal cutting image on the midline. Black arrow : whole ventricles become smaller and there is no more compression of the optic chiasm. B : Coronal cutting image on the optic chiasm. C : Axial cutting image on the cerebellar level. White arrow : the arachnoid cyst has completely disappeared in the cerebellum and the previously compressed fourth ventricle is released.
Reference
-
1. Al-Holou WN, Terman S, Kilburg C, Garton HJ, Muraszko KM, Maher CO. Prevalence and natural history of arachnoid cysts in adults. J Neurosurg. 2013; 118:222–231. PMID: 23140149.
Article2. Al-Holou WN, Yew AY, Boomsaad ZE, Garton HJ, Muraszko KM, Maher CO. Prevalence and natural history of arachnoid cysts in children. J Neurosurg Pediatr. 2010; 5:578–585. PMID: 20515330.
Article3. Arai H, Sato K, Wachi A, Okuda O, Takeda N. Arachnoid cysts of the middle cranial fossa : experience with 77 patients who were treated with cystoperitoneal shunting. Neurosurgery. 1996; 39:1108–1112. discussion 1112-1113. PMID: 8938764.4. Banna M. Arachnoid cysts on computed tomography. AJR Am J Roentgenol. 1976; 127:979–982. PMID: 998837.
Article5. Caemaert J, Abdullah J, Calliauw L, Carton D, Dhooge C, van Coster R. Endoscopic treatment of suprasellar arachnoid cysts. Acta Neurochir (Wien). 1992; 119:68–73. PMID: 1481755.
Article6. Choi JU, Kim DS, Huh R. Endoscopic approach to arachnoid cyst. Childs Nerv Syst. 1999; 15:285–291. PMID: 10461776.
Article7. Choi KY, Jung S, Kang SS, Kim IY, Jung TY, Jang WY. Technical considerations to prevent postoperative endocrine dysfunction after the fenestration of suprasellar arachnoid cyst. J Korean Neurosurg Soc. 2011; 49:262–266. PMID: 21716897.
Article8. Ciricillo SF, Cogen PH, Harsh GR, Edwards MS. Intracranial arachnoid cysts in children. A comparison of the effects of fenestration and shunting. J Neurosurg. 1991; 74:230–235. PMID: 1988593.
Article9. Eskandary H, Sabba M, Khajehpour F, Eskandari M. Incidental findings in brain computed tomography scans of 3000 head trauma patients. Surg Neurol. 2005; 63:550–553. discussion 553. PMID: 15936382.
Article10. Fewel ME, Levy ML, McComb JG. Surgical treatment of 95 children with 102 intracranial arachnoid cysts. Pediatr Neurosurg. 1996; 25:165–173. PMID: 9293543.
Article11. Galassi E, Tognetti F, Frank F, Fagioli L, Nasi MT, Gaist G. Infratentorial arachnoid cysts. J Neurosurg. 1985; 63:210–217. PMID: 4020444.
Article12. Gangemi M, Seneca V, Colella G, Cioffi V, Imperato A, Maiuri F. Endoscopy versus microsurgical cyst excision and shunting for treating intracranial arachnoid cysts. J Neurosurg Pediatr. 2011; 8:158–164. PMID: 21806357.
Article13. Halani SH, Safain MG, Heilman CB. Arachnoid cyst slit valves : the mechanism for arachnoid cyst enlargement. J Neurosurg Pediatr. 2013; 12:62–66. PMID: 23662935.
Article14. Hanieh A, Simpson DA, North JB. Arachnoid cysts : a critical review of 41 cases. Childs Nerv Syst. 1988; 4:92–96. PMID: 3401876.15. Harsh GR 4th, Edwards MS, Wilson CB. Intracranial arachnoid cysts in children. J Neurosurg. 1986; 64:835–842. PMID: 3701434.
Article16. Helland CA, Wester K. A population-based study of intracranial arachnoid cysts : clinical and neuroimaging outcomes following surgical cyst decompression in children. J Neurosurg. 2006; 105(5 Suppl):385–390. PMID: 17328263.
Article17. Hinojosa J, Esparza J, Muñoz MJ, Valencia J. [Endoscopic treatment of suprasellar arachnoid cysts]. Neurocirugia (Astur). 2001; 12:482–488. discussion 489. PMID: 11787396.18. Iacono RP, Labadie EL, Johnstone SJ, Bendt TK. Symptomatic arachnoid cyst at the clivus drained stereotactically through the vertex. Neurosurgery. 1990; 27:130–133. PMID: 2198483.
Article19. Katzman GL, Dagher AP, Patronas NJ. Incidental findings on brain magnetic resonance imaging from 1000 asymptomatic volunteers. JAMA. 1999; 282:36–39. PMID: 10404909.
Article20. Kim BS, Illes J, Kaplan RT, Reiss A, Atlas SW. Incidental findings on pediatric MR images of the brain. AJNR Am J Neuroradiol. 2002; 23:1674–1677. PMID: 12427622.21. Levy ML, Meltzer HS, Hughes S, Aryan HE, Yoo K, Amar AP. Hydrocephalus in children with middle fossa arachnoid cysts. J Neurosurg. 2004; 101(1 Suppl):25–31. PMID: 16206968.
Article22. Levy ML, Wang M, Aryan HE, Yoo K, Meltzer H. Microsurgical keyhole approach for middle fossa arachnoid cyst fenestration. Neurosurgery. 2003; 53:1138–1144. discussion 1144-1145. PMID: 14580280.
Article23. Oberbauer RW, Haase J, Pucher R. Arachnoid cysts in children : a European co-operative study. Childs Nerv Syst. 1992; 8:281–286. PMID: 1394268.24. Panigrahi S, Mishra SS, Das S, Patra SK, Satpathy PC. Large intradural craniospinal arachnoid cyst : a case report and review of literature. J Craniovertebr Junction Spine. 2012; 3:16–18. PMID: 23741124.
Article25. Pell MF, Thomas DG. The management of infratentorial arachnoid cyst by CT-directed stereotactic aspiration. Br J Neurosurg. 1991; 5:399–403. PMID: 1786136.
Article26. Pierre-Kahn A, Capelle L, Brauner R, Sainte-Rose C, Renier D, Rappaport R, et al. Presentation and management of suprasellar arachnoid cysts. Review of 20 cases. J Neurosurg. 1990; 73:355–359. PMID: 2200855.27. Raffel C, McComb JG. To shunt or to fenestrate : which is the best surgical treatment for arachnoid cysts in pediatric patients? Neurosurgery. 1988; 23:338–342. PMID: 3226511.
Article28. Sato H, Sato N, Katayama S, Tamaki N, Matsumoto S. Effective shunt-independent treatment for primary middle fossa arachnoid cyst. Childs Nerv Syst. 1991; 7:375–381. PMID: 1794117.
Article29. Starkman SP, Brown TC, Linell EA. Cerebral arachnoid cysts. J Neuropathol Exp Neurol. 1958; 17:484–500. PMID: 13564260.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Syringomyelia Associated with Posterior Fossa Arachnoid Cyst: Case Report
- Syringomyelia Associated with a Huge Retrocerebellar Arachnoid Cyst: A Case Report
- Two Cases of Arachnoid Cyst of the Middle Cranial Fossa
- Two Cases of Arachnoid Cyst of the Middle Cranial Fossa with Chronic Subdural Hematoma
- A Case of Prenatal diagnosis and Postnatal Treatment of Suprasellar Arachnoid Cyst
