Craniosynostosis : Updates in Radiologic Diagnosis
- Affiliations
-
- 1Department of Radiology, Daejeon St. Mary's Hospital, The Catholic University of Korea, Daejeon, Korea.
- 2Department of Radiology, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea.
- 3Department of Neurosurgery, Daejeon St. Mary's Hospital, The Catholic University of Korea, Daejeon, Korea. leeilwoo@catholic.ac.kr
- KMID: 2192091
- DOI: http://doi.org/10.3340/jkns.2016.59.3.219
Abstract
- The purpose of this article is to review imaging findings and to discuss the optimal imaging methods for craniosynostosis. The discussion of imaging findings are focused on ultrasonography, plain radiography, magnetic resonance imaging and computed tomography with 3-dimensional reconstruction. We suggest a strategy for imaging work-up for the diagnosis, treatment planning and follow-up to minimize or avoid ionized radiation exposure to children by reviewing the current literature.
Keyword
MeSH Terms
Figure
-
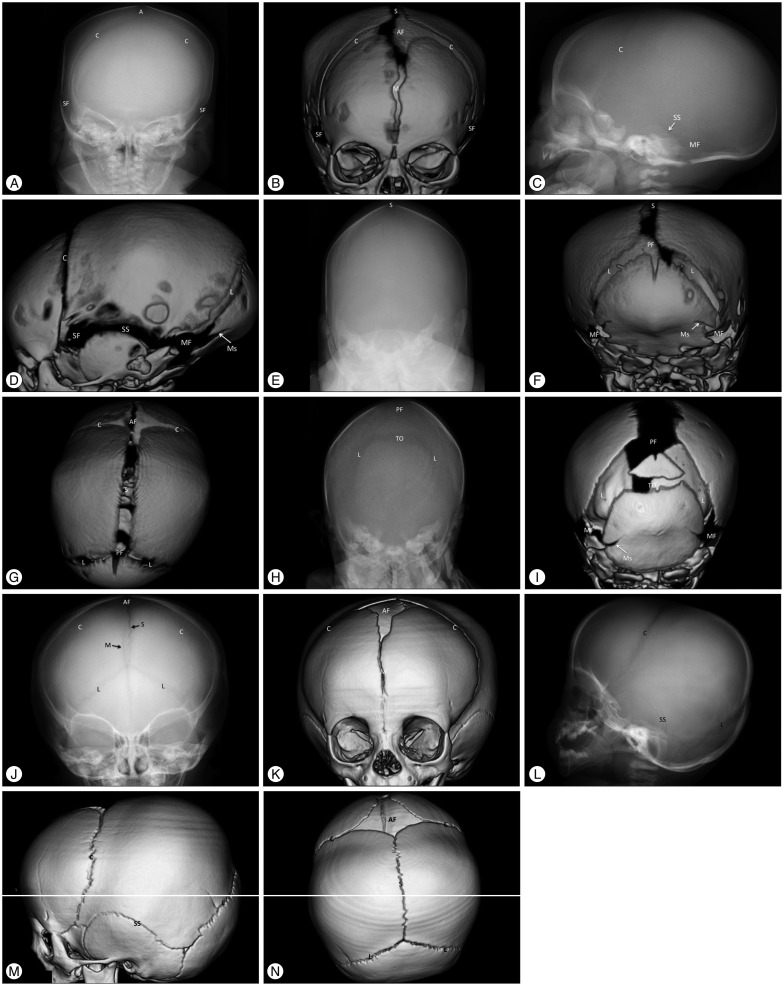
Fig. 1 Images of the normal anatomy of the cranial sutures of two neonates, 2 days (A–G) and 19 days (H and I) of age, and an infant at 12 months (J–N) of age using plain skull radiography and 3-dimensional (3-D) computed tomography (CT). Plain skull radiography images of the anterior-posterior (AP), lateral and posterior-anterior (PA) views are paired with 3-D CT images of the same direction. A and B are AP view images using plain skull radiography and 3-D CT, respectively; C and D are lateral view images; E and F are PA view images of a neonate at 2 days of age; H and I are PA images of a neonate at 19 days of age; and J-N are images of a 12-month-old boy. The superior view images (G and N) show only the 3-D CT images. Normal metopic (M), coronal (C), sagittal (S), lambdoid (L), mendosal (Ms), transverse occipital (TO), and squamosal (SS) sutures are demonstrated with a radiolucent, serrated and nonlinear appearance on plain and CT images. The anterior (AF), posterior (PF), sphenoidal (SF), and mastoid (MF) fontanels are also shown as radiolucent spaces. The typical radiolucent and serrated sutures become more distinct with age (comparing the images of the 2-day-old neonate with the images of the 12-month-old infant). The partially fused metopic suture, open AF and closed PF are normal at 12 months of age (J, K, and N). The cranial sutures of neonates have substantial variability. The distances between the bone plates of two the neonates are quite different normally (F and I), and the transverse occipital suture may or may not be seen in neonates (F and I). Neonatal sutures can be indistinct on plain skull radiography until 3 months after birth due to low thickness and low mineralization of the cranial bone, which impedes proper judgment of the state of the sutures. The metopic suture in A and the lambdoid sutures in C and E are indistinct in the lateral and PA images of the plain skull radiography. However, they are clearly demonstrated as patent sutures in the CT images (B, D, and F). Images of the normal anatomy of the cranial sutures of two neonates, 2 days (A–G) and 19 days (H and I) of age, and an infant at 12 months (J–N) of age using plain skull radiography and 3-dimensional (3-D) computed tomography (CT).
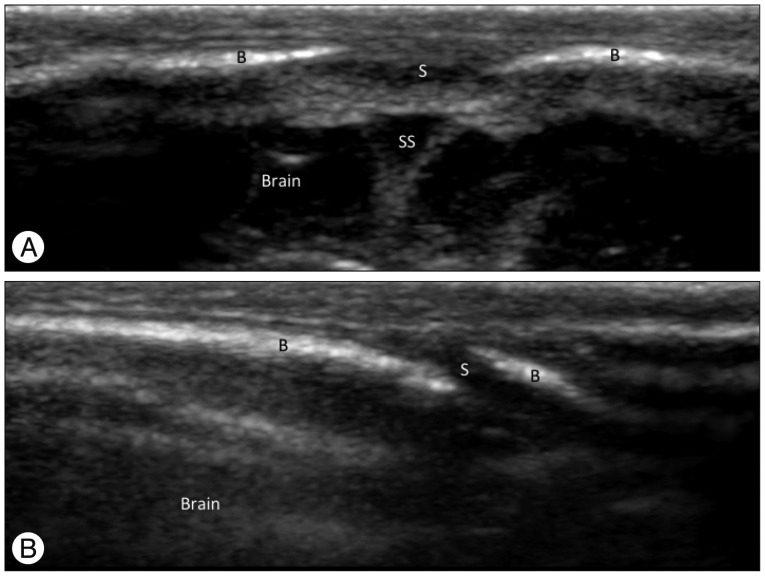
Fig. 2 Ultrasonographic findings of normal cranial sutures of a 2-day-old boy. A : A transverse sonogram of the sagittal suture shows the suture as a hypoechoic gap (S) between hyperechoic cranial bones (B) with end-to-end appearance. The superior sagittal sinus (SS) and the brain are noted under the skull. B : A transverse sonogram of the lambdoid suture shows the suture as a hypoechoic gap (S) between hyperechoic cranial bones (B) with a beveled appearance. This finding is also noted on ultrasonography of the coronal suture.
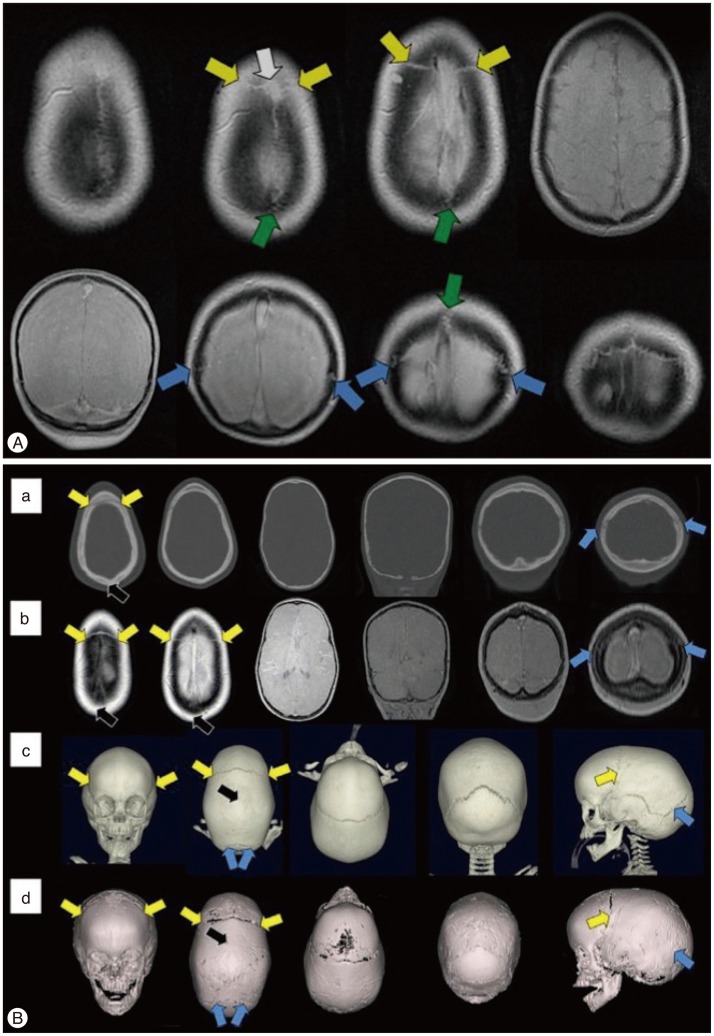
Fig. 3 Magnetic resonance imaging (MRI) findings of normal cranial sutures and craniosynostosis of children. A : Axial (top row) and coronal (bottom row) "Black Bone" imaging show normal patent cranial sutures as hyperintensity distinguished from the signal void of the cranial bones (Coronal suture : yellow arrow; Lambdoid suture : blue arrow; Sagittal suture : green arrow, visible anterior fontanelle : white arrow). B : Images of axial and coronal CT (a), axial and coronal "Black Bone" MRI (b), 3-D CT (c), and 3-D "Black Bone" MRI (d) show sagittal synostosis (Coronal suture : yellow arrow; Lambdoid suture : blue arrow; the site of synostosis : black arrow). Adapted from Eley KA, et al., Eur Radiol 24 : 2417-2426, 20146) with permission from Springer.
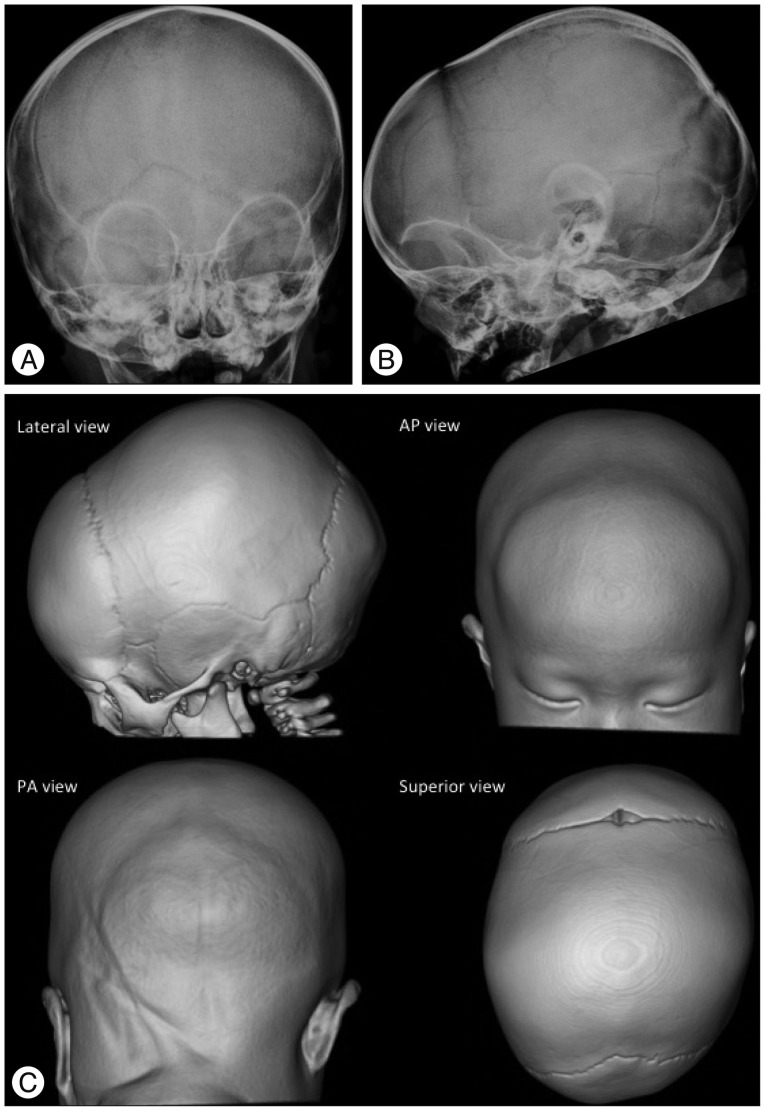
Fig. 4 Sagittal synostosis in an 11-month-old boy. The plain skull radiography (A : AP view, B : Lateral view) and 3-D CT images (C) show the absence of a radiolucent sagittal suture (A and C) and an elongated cranium with frontal bossing and occipital protrusion (B and C). The patent coronal and lambdoid sutures have a radiolucent, serrated and nonlinear appearance, and the fused metopic suture is normal in this 11-month-old baby.
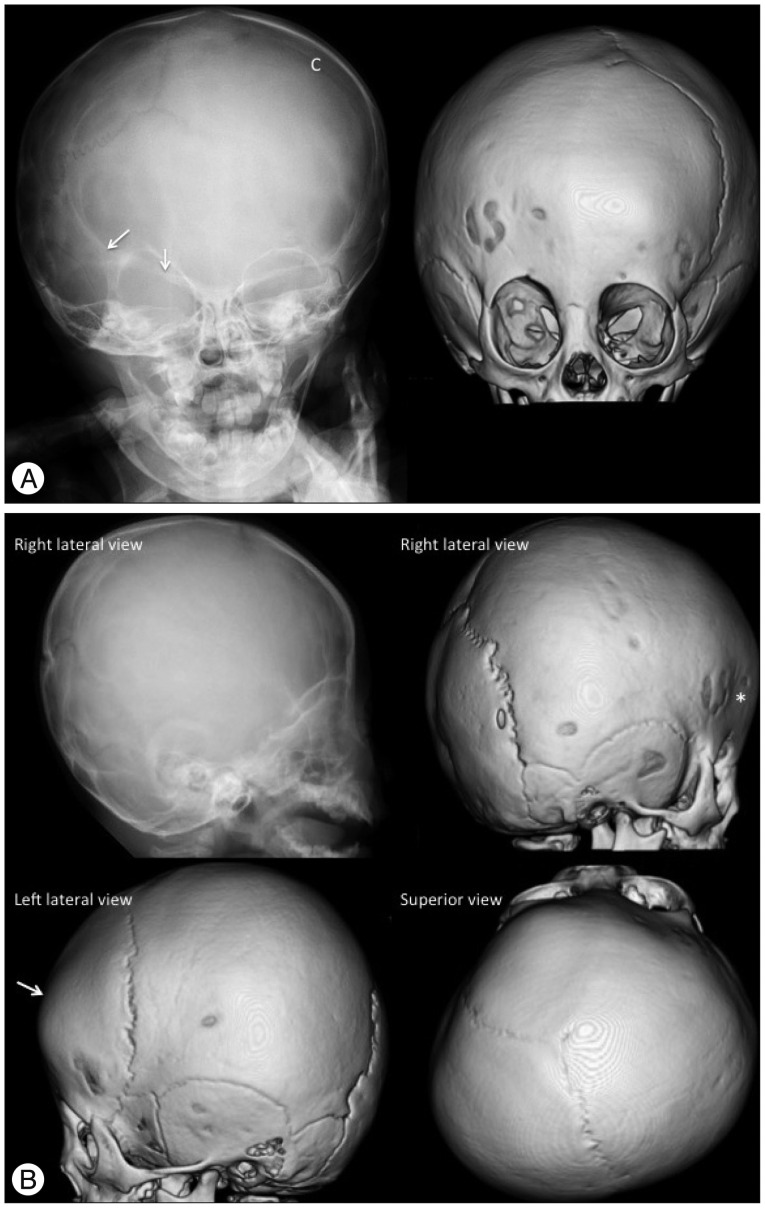
Fig. 5 Unicoronal (right) synostosis in a 12-month-old girl. A : The plain skull radiography and 3-D CT AP view images show the fused right coronal suture as the absence of a suture and a bony ridge compared to the patent left coronal suture (C). The "harlequin eye" appearance of the right orbit, the elevated ipsilateral sphenoid wings (arrows), the facial asymmetry (deviation of the nose and chin to the contralateral side), and the contralaterally shifted anterior fontanel are also demonstrated. The 3-D CT images also show the contralateral frontal bossing and ipsilateral hypoplastic supraorbital ridge. B : The plain skull radiography and 3-D CT lateral and superior view images show the absence of the right coronal suture, shallow ipsilateral anterior cranial fossa (*) and contralateral frontal bossing (arrow). Anterior plagiocephaly due to the decreased AP dimension of the right cranium with shifted anterior fontanel and contralateral frontal bossing are demonstrated on the superior view image.
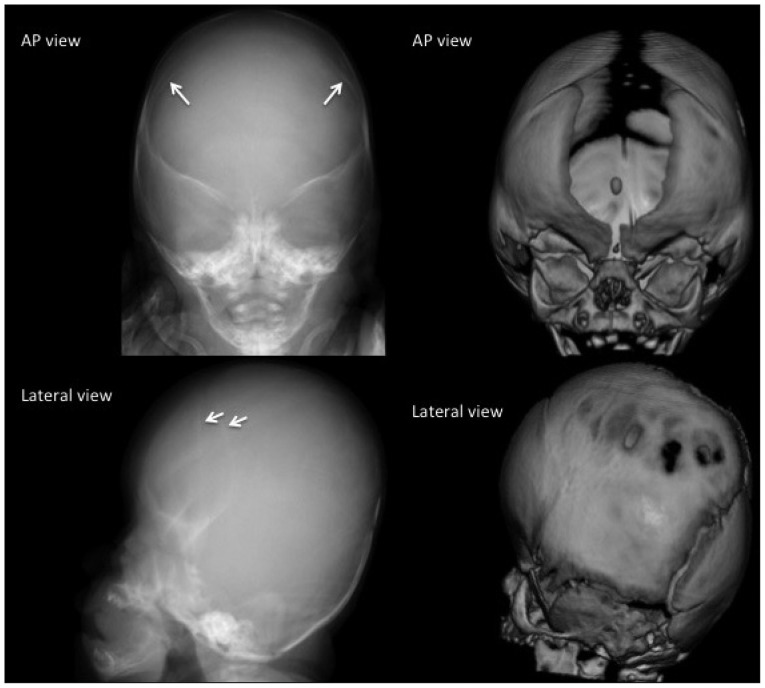
Fig. 6 Bicoronal synostosis in a 1-month-old boy. The fusion of both coronal sutures is demonstrated as sclerotic linear ridges (arrows). The patent metopic suture and anterior fontanel in this 1-month-old baby are normal. The plain radiography of this 1-month-baby does not show the wide open metopic suture. However, it demonstrates the sclerotic fused suture. Brachycephaly (short cranium by shortened AP and widened biparietal dimensions) and the bilateral "harlequin eye" deformity of the orbits combined with hypertelorism are characteristic of bicoronal synostosis.
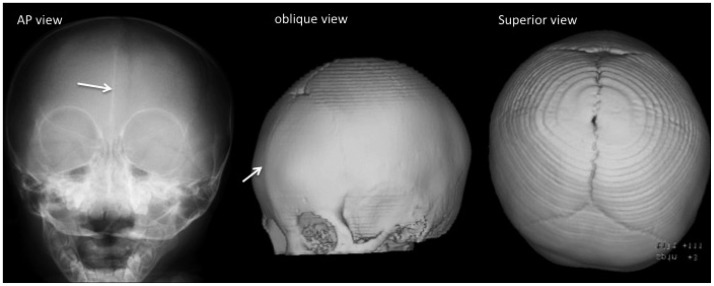
Fig. 7 Metopic synostosis in a 12-month-old boy. A fused metopic suture is demonstrated as a linear sclerotic line on the plain radiography image and a bony ridge on the 3-D CT image (arrows). Trigonocephaly, hypotelorism, a small ethmoid sinus, and the "quizzical eye" appearance of the orbits are noted.
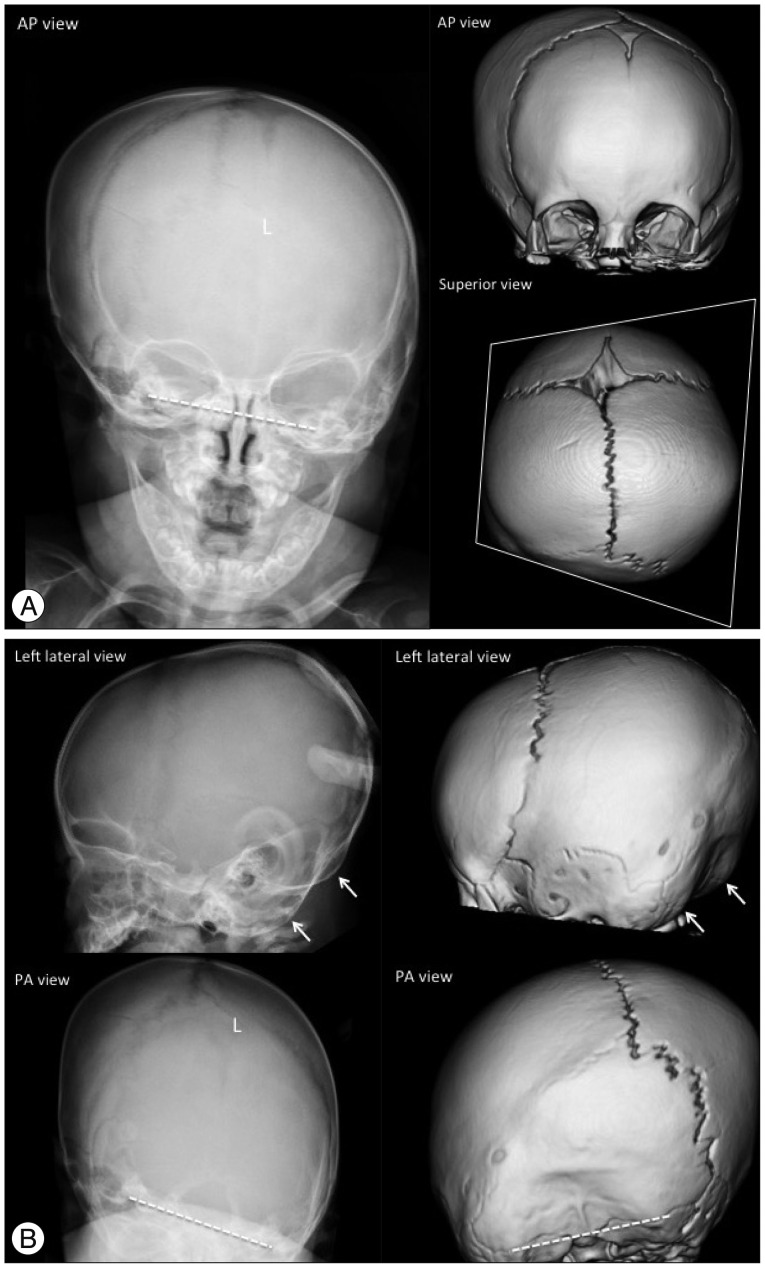
Fig. 8 Unilateral (left) lambdoid synostosis in an 8-month-old boy. The plain skull radiography and 3-D CT images show the fused suture as a partial absence of the suture with a linear ridge and perisutural sclerosis (L in A and B). Ipsilateral occipitoparietal flattening (posterior plagiocephaly), contralateral frontal and occipitoparietal bossing, and contralaterally shifted posterior fontanel are demonstrated. The cranium shows a trapezoidal configuration on the superior view image. The unilateral small posterior cranium makes a double contour of the occipital margin on the lateral view images (arrows in B), and the tilted skull base is noted in the AP and PA view images (dashed lines in A and B).
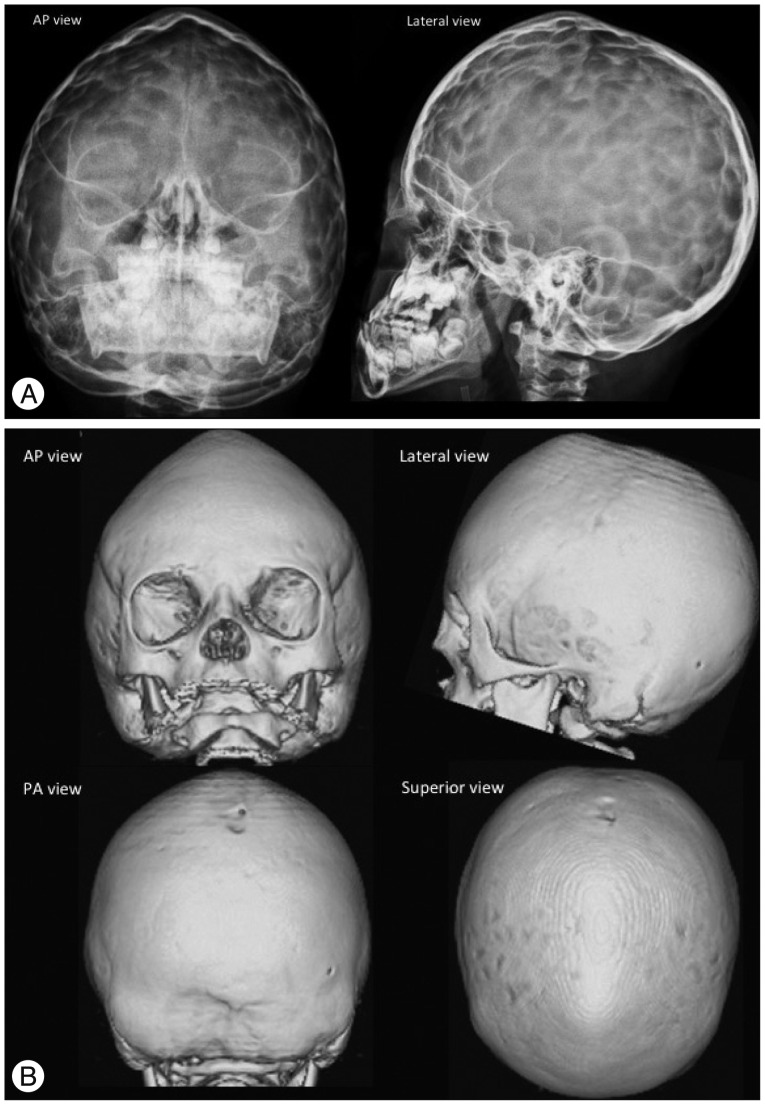
Fig. 9 Pansynostosis in a 10-month-old girl with Crouzon syndrome. The plain skull radiography (A) and 3-D CT (B) images show an absence of the coronal, sagittal and lambdoid sutures. The fontanels are also closed. The cranium is narrow and towered (oxycephaly). "Copper beaten" skull is also demonstrated on the plain radiography images (A) by gyral impressions on the inner table of the skull, which represents the increased intracranial pressure.
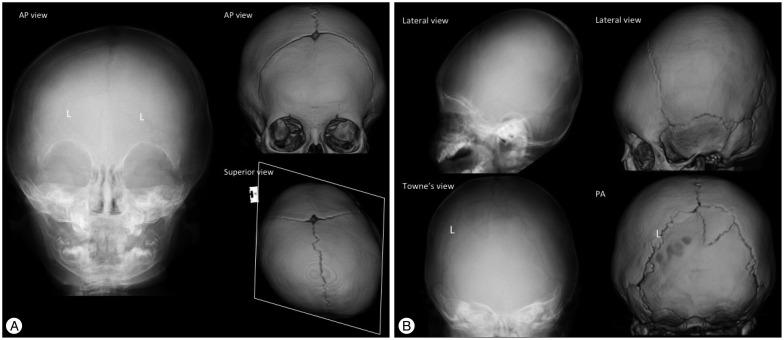
Fig. 10 Deformational plagiocephaly in a 10-month-old girl. Posterior plagiocephaly is seen on a superior view image of a 3-D CT due to left occipitoparietal flattening. However, both the lambdoid sutures (L) are patent with normal appearance and ipsilateral frontal bossing contrary to plagiocephaly caused by lambdoid craniosynostosis (A and B). The cranium shows a parallelogram configuration on the superior view image (A). The double contour of the occipital margin and the tilted skull based are not noted in deformational plagiocephaly (B).
Reference
-
1. Badve CA, K MM, Iyer RS, Ishak GE, Khanna PC. Craniosynostosis : imaging review and primer on computed tomography. Pediatr Radiol. 2013; 43:728–742. quiz 725-727. PMID: 23636536.
Article2. Branson HM, Shroff MM. Craniosynostosis and 3-dimensional computed tomography. Semin Ultrasound CT MR. 2011; 32:569–577. PMID: 22108219.
Article3. Calandrelli R, D'Apolito G, Gaudino S, Sciandra MC, Caldarelli M, Colosimo C. Identification of skull base sutures and craniofacial anomalies in children with craniosynostosis : utility of multidetector CT. Radiol Med. 2014; 119:694–704. PMID: 24510759.
Article4. Cohen MM Jr. Craniosynostosis and syndromes with craniosynostosis : incidence, genetics, penetrance, variability, and new syndrome updating. Birth Defects Orig Artic Ser. 1979; 15:13–63. PMID: 393319.5. Didier RA, Kuang AA, Schwartz DL, Selden NR, Stevens DM, Bardo DM. Decreasing the effective radiation dose in pediatric craniofacial CT by changing head position. Pediatr Radiol. 2010; 40:1910–1917. PMID: 20686761.
Article6. Eley KA, Watt-Smith SR, Sheerin F, Golding SJ. "Black Bone" MRI : a potential alternative to CT with three-dimensional reconstruction of the craniofacial skeleton in the diagnosis of craniosynostosis. Eur Radiol. 2014; 24:2417–2426. PMID: 25038852.
Article7. Ernst CW, Hulstaert TL, Belsack D, Buls N, Van Gompel G, Nieboer KH, et al. Dedicated sub 0.1 mSv 3DCT using MBIR in children with suspected craniosynostosis : quality assessment. Eur Radiol. 2016; 26:892–899. PMID: 26123408.
Article8. Jaffurs D, Denny A. Diagnostic pediatric computed tomographic scans of the head : actual dosage versus estimated risk. Plast Reconstr Surg. 2009; 124:1254–1260. PMID: 19935310.
Article9. Kaasalainen T, Palmu K, Lampinen A, Reijonen V, Leikola J, Kivisaari R, et al. Limiting CT radiation dose in children with craniosynostosis : phantom study using model-based iterative reconstruction. Pediatr Radiol. 2015; 45:1544–1553. PMID: 25939873.
Article10. Kirmi O, Lo SJ, Johnson D, Anslow P. Craniosynostosis : a radiological and surgical perspective. Semin Ultrasound CT MR. 2009; 30:492–512. PMID: 20099636.11. Lenton KA, Nacamuli RP, Wan DC, Helms JA, Longaker MT. Cranial suture biology. Curr Top Dev Biol. 2005; 66:287–328. PMID: 15797457.
Article13. Nagaraja S, Anslow P, Winter B. Craniosynostosis. Clin Radiol. 2013; 68:284–292. PMID: 22939693.
Article14. Persing JA, Jane JA, Shaffrey M. Virchow and the pathogenesis of craniosynostosis : a translation of his original work. Plast Reconstr Surg. 1989; 83:738–742. PMID: 2648432.15. Regelsberger J, Delling G, Helmke K, Tsokos M, Kammler G, Kränzlein H, et al. Ultrasound in the diagnosis of craniosynostosis. J Craniofac Surg. 2006; 17:623–625. discussion 626-628. PMID: 16877903.
Article16. Schweitzer T, Böhm H, Meyer-Marcotty P, Collmann H, Ernestus RI, Krauß J. Avoiding CT scans in children with single-suture craniosynostosis. Childs Nerv Syst. 2012; 28:1077–1082. PMID: 22349960.
Article17. Schweitzer T, Kunz F, Meyer-Marcotty P, Müller-Richter UD, Böhm H, Wirth C, et al. Diagnostic features of prematurely fused cranial sutures on plain skull X-rays. Childs Nerv Syst. 2015; 31:2071–2080. PMID: 26298825.
Article18. Slater BJ, Lenton KA, Kwan MD, Gupta DM, Wan DC, Longaker MT. Cranial sutures: a brief review. Plast Reconstr Surg. 2008; 121:170e–178e.
Article19. Soboleski D, McCloskey D, Mussari B, Sauerbrei E, Clarke M, Fletcher A. Sonography of normal cranial sutures. AJR Am J Roentgenol. 1997; 168:819–821. PMID: 9057541.
Article20. Soboleski D, Mussari B, McCloskey D, Sauerbrei E, Espinosa F, Fletcher A. High-resolution sonography of the abnormal cranial suture. Pediatr Radiol. 1998; 28:79–82. PMID: 9472048.
Article21. Sze RW, Parisi MT, Sidhu M, Paladin AM, Ngo AV, Seidel KD, et al. Ultrasound screening of the lambdoid suture in the child with posterior plagiocephaly. Pediatr Radiol. 2003; 33:630–636. PMID: 12879318.
Article22. Vazquez JL, Pombar MA, Pumar JM, del Campo VM. Optimised low-dose multidetector CT protocol for children with cranial deformity. Eur Radiol. 2013; 23:2279–2287. PMID: 23504037.
Article23. Weinzweig J, Kirschner RE, Farley A, Reiss P, Hunter J, Whitaker LA, et al. Metopic synostosis : Defining the temporal sequence of normal suture fusion and differentiating it from synostosis on the basis of computed tomography images. Plast Reconstr Surg. 2003; 112:1211–1218. PMID: 14504503.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Update of Diagnostic Evaluation of Craniosynostosis with a Focus on Pediatric Systematic Evaluation and Genetic Studies
- Genetic Syndromes Associated with Craniosynostosis
- Current and Future Perspectives in Craniosynostosis
- Unilateral Lambdoid Craniosynostosis in a Twin-to-Twin Transfusion Syndrome Donor: A Case Report
- Moleculobiological Analysis of Fibroblast Growth Factor Receptors in Korean Patients with Craniosynostosis
