Protocol Based Real-Time Continuous Electroencephalography for Detecting Vasospasm in Subarachnoid Hemorrhage
- Affiliations
-
- 1Department of Neurology, Keimyung University Dongsan Medical Center, Daegu, Korea.
- 2Department of Neurosurgery, Seoul National University Bundang Hospital, Seongnam, Korea.
- 3Department of Neurology, Seoul National University Bundang Hospital, Seongnam, Korea. mkhan@snu.ac.kr
- KMID: 2192046
- DOI: http://doi.org/10.3340/jkns.2016.59.2.154
Abstract
- A continuous electroencephalography (cEEG) can be helpful in detecting vasospasm and delayed cerebral ischemia in aneurysmal subarachnoid hemorrhage (SAH). We describe a patient with an aneurysmal SAH whose symptomatic vasospasm was detected promptly by using a real-time cEEG. Patient was immediately treated by intraarterial vasodilator therapy. A 50-year-old woman without any significant medical history presented with a severe bifrontal headache due to acute SAH with a ruptured aneurysm on the anterior communicating artery (Fisher grade 3). On bleed day 6, she developed a sudden onset of global aphasia and left hemiparesis preceded by cEEG changes consistent with vasospasm. A stat chemical dilator therapy was performed and she recovered without significant neurological deficits. A real-time and protocol-based cEEG can be utilized in order to avoid any delay in detection of vasospasm in aneurysmal SAH and thereby improve clinical outcomes.
Keyword
MeSH Terms
Figure
-
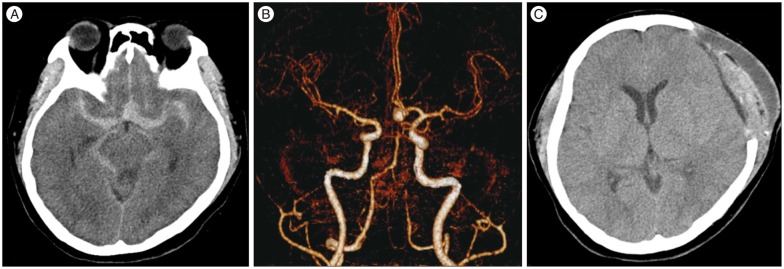
Fig. 1 Brain CT and CTA. Initial brain CT (A) and CTA (B) showing a diffuse subarachnoid hemorrhage without intraventricular hemorrhage (Fisher grade 3) and a wide-neck aneurysm of 7.3×6 mm at the anterior communicating artery. Follow-up CT on post-bleed day 11 (C) shows mild epi- and sub-dural hematoma but no ischemic stroke.

Fig. 2 Quantitative continuous EEG. Quantitative continuous EEG data from two bipolar channels in the bilateral fronto-central (F3-C3, F4-C4) and centro-parietal (C3-P3, C4-P4) regions showing progressive decrement of the alpha-delta ratio after 10 a.m. on the left hemisphere with more prominence on the centro-parietal than fronto-central region, and an increase of alpha-delta ratio after intra-arterial chemical angioplasty (A and B). Raw EEG data just before angioplasty, showing the rise in asymmetry with delta slowing on the left hemisphere (C). Ratio : alpha-to-delta ratio, DSA : density spectral array, EEG : electroencephalogram, aEEG : amplitude EEG.

Fig. 3 Digital subtraction angiography before and after chemical angioplasty. On post-bleed day 6, a first conventional angiography before chemical angioplasty (A) shows severe vasospasm in the anterior cerebral artery and middle cerebral artery of the left hemisphere and a residual sac on the clipped aneurysm. Conventional angiography after chemical angioplasty with 4 mg nimodipine (B) shows an increase in middle cerebral artery caliber. On post-bleed day 8, final conventional angiography before chemical angioplasty (C) shows that moderate vasospasm on the left middle cerebral artery remains, and that vasospasm improves after chemical angioplasty with 5 mg nimodipine (D).
Reference
-
1. Claassen J, Hirsch LJ, Kreiter KT, Du EY, Connolly ES, Emerson RG, et al. Quantitative continuous EEG for detecting delayed cerebral ischemia in patients with poor-grade subarachnoid hemorrhage. Clin Neurophysiol. 2004; 115:2699–2710. PMID: 15546778.
Article2. Connolly ES Jr, Rabinstein AA, Carhuapoma JR, Derdeyn CP, Dion J, Higashida RT, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage : a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2012; 43:1711–1737. PMID: 22556195.
Article3. Dankbaar JW, de Rooij NK, Velthuis BK, Frijns CJ, Rinkel GJ, van der Schaaf IC. Diagnosing delayed cerebral ischemia with different CT modalities in patients with subarachnoid hemorrhage with clinical deterioration. Stroke. 2009; 40:3493–3498. PMID: 19762703.
Article4. Foreman B, Claassen J. Quantitative EEG for the detection of brain ischemia. Crit Care. 2012; 16:216. PMID: 22429809.
Article5. Frontera JA, Claassen J, Schmidt JM, Wartenberg KE, Temes R, Connolly ES Jr, et al. Prediction of symptomatic vasospasm after subarachnoid hemorrhage : the modified fisher scale. Neurosurgery. 2006; 59:21–27. discussion 21-27PMID: 16823296.
Article6. Jordan KG. Emergency EEG and continuous EEG monitoring in acute ischemic stroke. J Clin Neurophysiol. 2004; 21:341–352. PMID: 15592008.7. Kim SS, Park DH, Lim DJ, Kang SH, Cho TH, Chung YG. Angiographic features and clinical outcomes of intra-arterial nimodipine injection in patients with subarachnoid hemorrhage-induced vasospasm. J Korean Neurosurg Soc. 2012; 52:172–178. PMID: 23115657.
Article8. Macdonald RL, Rosengart A, Huo D, Karrison T. Factors associated with the development of vasospasm after planned surgical treatment of aneurysmal subarachnoid hemorrhage. J Neurosurg. 2003; 99:644–652. PMID: 14567598.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Relation between Thromboembolism and Delayed Ischemic Neurological Deficits in Aneurysmal Subarachnoid Hemorrhage
- The Relationship Between CT Findings and Cerebral Vasospasm in Cerebral Aneursms
- Evaluation of Subarachnoid Hemorrhage due to Aneurysmal Rupture and Cerebral Vasospasm by CT
- Factors Related to Clinical Vasospasm after Aneurysmal Subarachnoid Hemorrhage
- Transcranial Doppler Monitoring in Subarachnoid Hemorrhage
