Intractable Hiccup as the Presenting Symptom of Cavernous Hemangioma in the Medulla Oblongata: A Case Report and Literature Review
- Affiliations
-
- 1Department of Pathology, Chonnam National University Research Institute of Medical Sciences, Chonnam National University Hwasun Hospital & Medical School, Hwasun, Korea.
- 2Department of Neurosurgery, Chonnam National University Research Institute of Medical Sciences, Chonnam National University Hwasun Hospital & Medical School, Hwasun, Korea. moonks@chonnam.ac.kr
- 3Department of Radiology, Chonnam National University Research Institute of Medical Sciences, Chonnam National University Hwasun Hospital & Medical School, Hwasun, Korea.
- KMID: 2191122
- DOI: http://doi.org/10.3340/jkns.2014.55.6.379
Abstract
- A case of intractable hiccup developed by cavernous hemangioma in the medulla oblongata is reported. There have been only five previously reported cases of medullary cavernoma that triggered intractable hiccup. The patient was a 28-year-old man who was presented with intractable hiccup for 15 days. It developed suddenly, then aggravated progressively and did not respond to any types of medication. On magnetic resonance images, a well-demarcated and non-enhancing mass with hemorrhagic changes was noted in the left medulla oblongata. Intraoperative findings showed that the lesion was fully embedded within the brain stem and pathology confirmed the diagnosis of cavernous hemangioma. The hiccup resolved completely after the operation. Based on the presumption that the medullary cavernoma may trigger intractable hiccup by displacing or compression the hiccup arc of the dorsolateral medulla, surgical excision can eliminate the symptoms, even in the case totally buried in brainstem.
Keyword
Figure
-
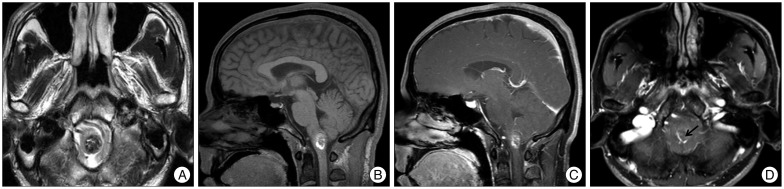
Fig. 1 Preoperative MRI. A : Axial T2-weighted image shows a nodular lesion in the left sided cervicomedullary junction, with marked hyposignal intensity containing internal foci of hypersignal intensity. Sagittal pre- (B) and post- (C) gadolinium T1WI images show a non-enhancing cavernous hemangioma surrounded by bright hypersignal intensity halo which is consistent with blood products. D : An associated small developmental venous anomaly (arrow) is visualized in superior aspect of the cavernous hemangioma on axial post-gadolinium T1WI image.
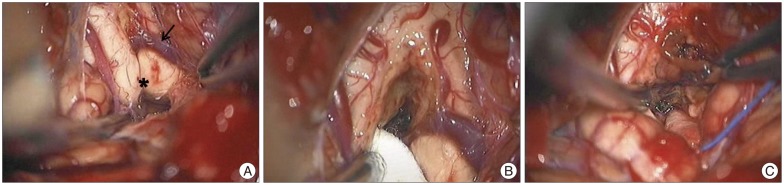
Fig. 2 Peroperative photographs (A) demonstrating slightly bulged medulla oblongata with superficial abnormal draining vein (arrow). Note that the mass was located caudally to obex and removed using hemosiderin plane between hemangioma and normal parenchyme (B and C). *: obex.
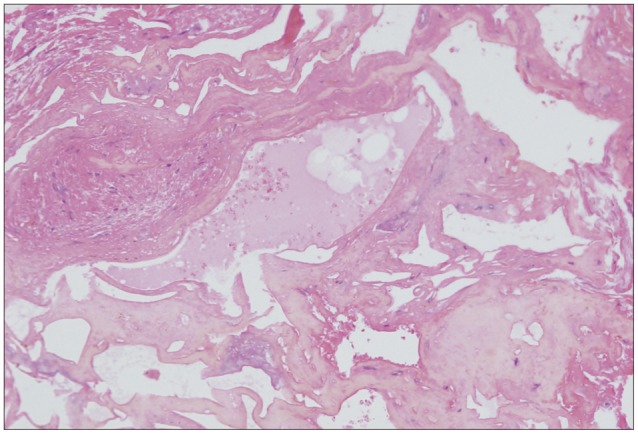
Fig. 3 Microscopic findings of the medullary cavernous hemangioma. Histopathologic exam reveals a typical cavernous hemangioma with irregularly dilated vascular spaces. The vascular walls are accompanied by cautery artifacts (hematoxylin-eosin, original magnification, ×200).
Cited by 1 articles
-
Hiccups in neurocritical care
Vanitha Rajagopalan, Deep Sengupta, Keshav Goyal, Surya Kumar Dube, Ashish Bindra, Shweta Kedia
J Neurocrit Care. 2021;14(1):18-28. doi: 10.18700/jnc.200018.
Reference
-
1. Abla AA, Lekovic GP, Turner JD, de Oliveira JG, Porter R, Spetzler RF. Advances in the treatment and outcome of brainstem cavernous malformation surgery : a single-center case series of 300 surgically treated patients. Neurosurgery. 2011; 68:403–414. discussion 414-415. PMID: 21654575.2. al Deeb SM, Sharif H, al Moutaery K, Biary N. Intractable hiccup induced by brainstem lesion. J Neurol Sci. 1991; 103:144–150. PMID: 1880531.
Article3. Arita H, Oshima T, Kita I, Sakamoto M. Generation of hiccup by electrical stimulation in medulla of cats. Neurosci Lett. 1994; 175:67–70. PMID: 7970214.
Article4. Eisenächer A, Spiske J. Persistent hiccups (singultus) as the presenting symptom of medullary cavernoma. Dtsch Arztebl Int. 2011; 108:822–826. PMID: 22211149.
Article5. Hassler R. Die neuronalen system der extrapyramidalen myoclonien und deren stereotaktische behandlung. In : Doose H, editor. Aktuelle Neuropadiatrie. Stuttgart: Thieme;1997. p. 20–46.6. Johnson DL. Intractable hiccups : treatment by microvascular decompression of the vagus nerve. Case Report. J Neurosurg. 1993; 78:813–816. PMID: 8468612.
Article7. Kumral E, Acarer A. Primary medullary haemorrhage with intractable hiccup. J Neurol. 1998; 245:620–622. PMID: 9758303.
Article8. Lapresle J, Hamida MB. The dentato-olivary pathway. Somatotopic relationship between the dentate nucleus and the contralateral inferior olive. Arch Neurol. 1970; 22:135–143. PMID: 4188259.9. Launois S, Bizec JL, Whitelaw WA, Cabane J, Derenne JP. Hiccup in adults : an overview. Eur Respir J. 1993; 6:563–575. PMID: 8491309.10. Matsuo F, Ajax ET. Palatal myoclonus and denervation supersensitivity in the central nervous system. Ann Neurol. 1979; 5:72–78. PMID: 34357.
Article11. Mattana M, Mattana PR, Roxo MR. Intractable hiccup induced by cavernous angioma in the medulla oblongata : case report. J Neurol Neurosurg Psychiatry. 2010; 81:353–354. PMID: 20185478.
Article12. Musumeci A, Cristofori L, Bricolo A. Persistent hiccup as presenting symptom in medulla oblongata cavernoma : a case report and review of the literature. Clin Neurol Neurosurg. 2000; 102:13–17. PMID: 10717396.
Article13. Oshima T, Sakamoto M, Tatsuta H, Arita H. GABAergic inhibition of hiccup-like reflex induced by electrical stimulation in medulla of cats. Neurosci Res. 1998; 30:287–293. PMID: 9678632.
Article14. Park MH, Kim BJ, Koh SB, Park MK, Park KW, Lee DH. Lesional location of lateral medullary infarction presenting hiccups (singultus). J Neurol Neurosurg Psychiatry. 2005; 76:95–98. PMID: 15608002.
Article15. Pechlivanis I, Seiz M, Barth M, Schmieder K. A healthy man with intractable hiccups. J Clin Neurosci. 2010; 17:781–783. PMID: 20359895.
Article16. Porter RW, Detwiler PW, Spetzler RF, Lawton MT, Baskin JJ, Derksen PT, et al. Cavernous malformations of the brainstem : experience with 100 patients. J Neurosurg. 1999; 90:50–58. PMID: 10413155.17. Stotka VL, Barcay SJ, Bell HS, Clare FB. Intractable hiccough as the primary manifestation of brain stem tumor. Am J Med. 1962; 32:312–315. PMID: 13917547.
Article18. Thaci B, Burns JD, Delalle I, Vu T, Davies KG. Intractable hiccups resolved after resection of a cavernous malformation of the medulla oblongata. Clin Neurol Neurosurg. 2013; 115:2247–2250. PMID: 23932467.
Article19. Turazzi S, Alexandre A, Bricolo A, Rizzuto N. Opsoclonus and palatal myoclonus during prolonged post-traumatic coma. A clinico-pathologic study. Eur Neurol. 1977; 15:257–263. PMID: 913438.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Intractable Hiccups as Presenting Symptom of Multiple Sclerosis
- A Case of Rhombencephalitis Presented with Intractable Hiccup
- Extracerebral Cavernous Hemangioma of the Middle Cranial Fossa: Report of 2 Cases and Review of Literature
- Two Cases of the Cavernous Hemangioma of the Scrotum
- A Case of Cavernous Hemangioma of the Bulbar Conjunctiva
