Results of Operative Treatment for a Bone Cyst in the Proximal Femur
- Affiliations
-
- 1Department of Orthopedic Surgery, Research Institute of Clinical Medicine, Chonbuk National University School of Medicine, Jeonju, Korea.
- 2Department of Orthopedic Surgery, Gwangju Veterans Hospital, Gwangju, Korea. chm1228@hanmail.net
- 3Department of Orthopedic Surgery, Busan Veterans Hospital, Busan, Korea.
- KMID: 2190776
- DOI: http://doi.org/10.5371/jkhs.2011.23.1.54
Abstract
- PURPOSE
We retrospectively evaluated performing curettage and bone grafting for the treatment of simple bone cyst in 21 patients with cysts in the proximal femur. The purpose of this study was to review the results with a minimum follow up of 24 months.
MATERIALS AND METHODS
We treated 21 cases of simple bone cysts with curettage and a bone graft from June 1995 to July 2008. 4 male and 17 female patients (age range: 14~62 years (mean age: 39.8 years) volunteered for this study. The range of the follow-up period was from 24 months to 6 years (mean follow-up: 63.7 months). We evaluated the effect of treatment by examining the simple follow-up radiographs according to Oppenheim's classification. We retrospectively reviewed the site of the cysts, the patients' ages at the time of the diagnosis, the incidence of pathologic fracture, the association with femoro-acetabular impingement (FAI) and the type of bone graft.
RESULTS
The investigation revealed that 20 out of 21 patients had better than improved results. 14 patients of the 15 patients who were treated with an autogenous bone graft had better than improved results and all 6 patients who received an autogenous and allergenic bone graft had better than improved results. Two patients had associated FAI. These cases were managed with arthroscopic labral trimming and curettage. There were no specific complications related to the bone cyst and the operative procedure.
CONCLUSION
We believe curettage and bone grafting and stabilization with compression hip screws is a reasonable treatment for simple bone cysts in the proximal femur. The bone cyst in the femoral head neck junction in patients older than 50 years old is related with femoroacetabular impingement.
Keyword
MeSH Terms
Figure
-
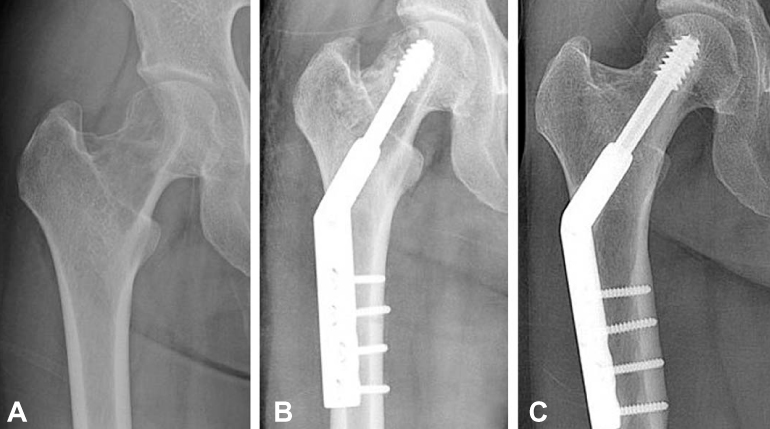
Fig. 1 Radiographs of a 29 year-old female who presented with right hip pain. (A) The bony cyst is mainly located in the head and neck region. (B) Radiographs taken after the operation (Fixation with compression hip screw after curettage and autogenous bone graft). (C) AP views taken 36 months after operation.

Fig. 2 Radiographs of a 62-year-old female who presented with right hip pain. (A) The bony cyst is mainly located in the neck region but partly involves the femoral head. (B) Magnetic resonance image of the right hip, an intraosseous cyst (herniation fit) can be seen to the anterosuperoir aspect of the femoral head-neck junction and pincer type FAI also. (C) Radiographs taken after operation (Fixation with compression hip screw after curettage and autogenous bone graft). (D) AP views taken 28 months after operation.
Reference
-
1. Capanna R, Campanacci DA, Manfrini M. Unicameral and aneurismal bone cysts. Orthop Clin North Am. 1996. 27:605–614.2. Ganz R, Parvizi J, Beck M, Leunig M, Nötzli H, Siebenrock KA. Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res. 2003. 417:112–120.3. Killian JT, Wilkinson L, White S, Brassard M. Treatment of unicameral bone cyst with demineralized bone matrix. J Pediatr Orthop. 1998. 18:621–624.
Article4. Oppenheim WL, Galleno H. Operative treatment versus steroid injection in the management of unicameral bone cysts. J Pediatr Orthop. 1984. 4:1–7.
Article5. Capanna R, Dal Monte A, Gitelis S, Campanacci M. The natural history of unicameral bone cyst after steroid injection. Clin Orthop Relat Res. 1982. 166:204–211.
Article6. Goel AR, Kriger J, Bronfman R, Lauf E. Unicameral bone cysts: treatment with methylprednisone acetate injections. J Foot Ankle Surg. 1994. 33:6–15.7. Springfield DS. Morrissy RT, Weinstein SL, editors. Bone and soft tissue tumors. 1996. Philadelphia: Lippincott-Raven;448–450.8. Chigira M, Takehi Y, Nagase M, Arita S, Shimizu T, Shinozaki T. A case of multiple simple bone cysts. With special reference to their etiology and treatment. Arch Orthop Trauma Surg. 1987. 106:390–393.9. Pitt MJ, Graham AR, Shipman JH, Birkby W. Herniation pit of the femoral neck. AJR Am J Roentgenol. 1982. 138:1115–1121.
Article10. Leunig M, Beck M, Kalhor M, Kim YJ, Werlen S, Ganz R. Fibrocystic changes at anterosuperior femoral neck: prevalence in hips with femoroacetabular impingement. Radiology. 2005. 236:237–246.
Article11. Chigira M, Maehara S, Arita S, Udagawa E. The etiology and treatment of simple bone cysts. J Bone Joint Surg Br. 1983. 65:633–637.12. Shinozaki T, Arita S, Watanabe H, Chigira M. Simple bone cysts treated by multiple drill-holes. 23 cysts followed 2-10 years. Acta Orthop Scand. 1996. 67:288–290.
Article13. Campanacci M, Capanna R, Picci P. Unicameral and aneurysmal bone cysts. Clin Orthop Relat Res. 1986. 204:25–36.
Article14. Spence KF Jr, Bright RW, Fitzgerald SP, Sell KW. Solitary unicameral bone cyst: treatment with freeze-dried crushed cortical-bone allograft. A review of one hundred and forty-four cases. J Bone Joint Surg Am. 1976. 58:636–641.15. Jaffe KA, Dunham WK. Treatment of benign lesions of the femoral head and neck. Clin Orthop Relat Res. 1990. 257:134–137.
Article16. Günther KP, Hartmann A, Aikele P, Aust D, Ziegler J. Large femoral-neck cysts in association with femoroacetabular impingement. A report of three cases. J Bone Joint Surg Am. 2007. 89:863–870.
Article17. Kaelin AJ, MacEwen GD. Unicameral bone cysts. Natural history and the risk of fracture. Int Orthop. 1989. 13:275–282.18. Shih HN, Cheng CY, Chen YJ, Huang TJ, Hsu RW. Treatment of the femoral neck and trochanteric benign lesions. Clin Orthop Relat Res. 1996. 328:220–226.
Article19. Stürz H, Zenker H, Buckl H. Total subperiosteal resection treatment of solitary bone cysts of the humerus. Arch Orthop Trauma Surg. 1979. 93:231–239.
Article20. Neer CS 2nd, Francis KC, Marcove RC, Terz J, Carbonara PN. Treatment of unicameral bone cyst. A follow-up study of one hundred seventy-five cases. J Bone Joint Surg Am. 1966. 48:731–745.21. Spence KF, Sell KW, Brown RH. Solitary bone cyst: treatment with freeze-dried cancellous bone allograft. A study of one hundred seventy-seven cases. J Bone Joint Surg Am. 1969. 51:87–96.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Solitary Bone Cyst of the Proximal Femur Mimicking Fibrous Dysplasia: A Case Report
- A Case of Unicameral Bone Cyst with Fracture of Femoral Neck
- Early Result of Demineralized Bone Matrix (DBM, Genesis(R)) in Bone Defect after Operative Treatment of Benign Bone Tumor
- The Treatment of Pathologic Troehanterie Fracture of the Femur by Solitary Bone Cyst in Children
- Treatment of Simple Bone Cyst
