Anterior Approaches in Hip Surgery
- Affiliations
-
- 1Institute for Skeletal Aging, Department of Orthopaedic Surgery, College of Medicine, Hallym University, Chuncheon, Korea. totalhip@hallym.ac.kr
- KMID: 2190719
- DOI: http://doi.org/10.5371/jkhs.2011.23.2.95
Abstract
- The Smith-Petersen anterior approach and the Watson-Jones anterolateral approach are the two most renowned anterior approaches for hip surgery. The anterior approach offers several advantages, including a reduced dislocation risk as compared with that associated with the posterior approach. The post-operative dislocation rate after total hip arthroplasty is known to be 2~3 times lower than that of the posterior approach. However, a more extensive skin incision and poor anatomical visualization are some of the disadvantages of the anterior approach. Nevertheless, since this approach preserves the circulation to the femoral head, the ability to perform the anterior approach is imperative for hip surgeons.
Keyword
MeSH Terms
Figure
-
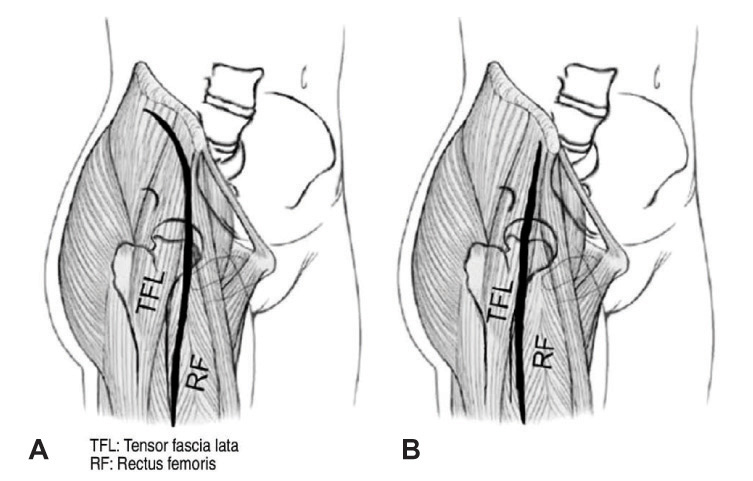
Fig. 1 (A) Anterior approach: Smith-Petersen incision. The distal incision splits between the tensor and the sartorius muscles. (B) Anterior approach modification: Hueter. The dissection mimics the distal portion of the Smith-Petersen approach.
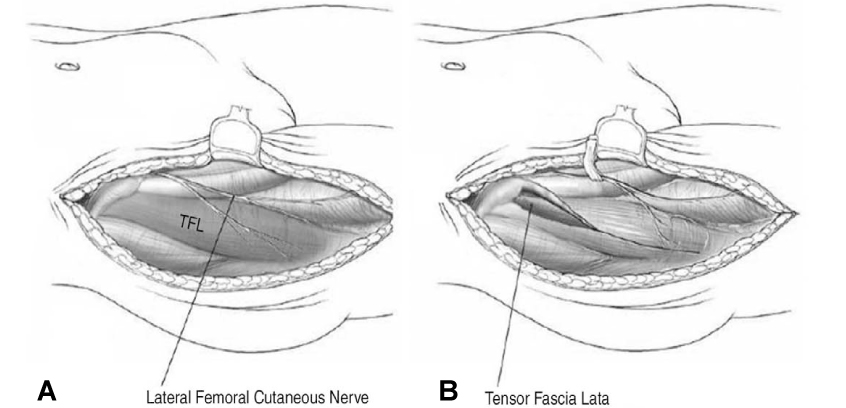
Fig. 2 Anterior approach: Branches of the lateral femoral cutaneous nerve may interfere with the anterior approach as they extend across the line of deep dissection between the tensor and sartorius muscles. The main trunk of this nerve should be identified and retracted medially.
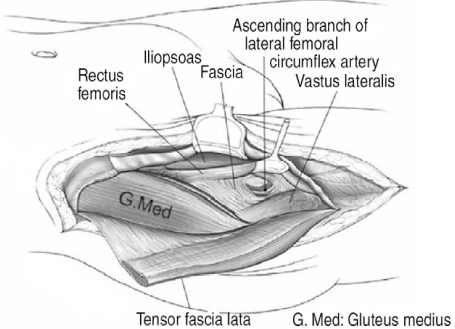
Fig. 3 Anterior approach: Tensor has been released from its origin to expose the gluteus medius. The ascending branch of the lateral femoral circumflex can be found in the deep tissue between the gluteus medius and the rectus femoris (deep retractor).
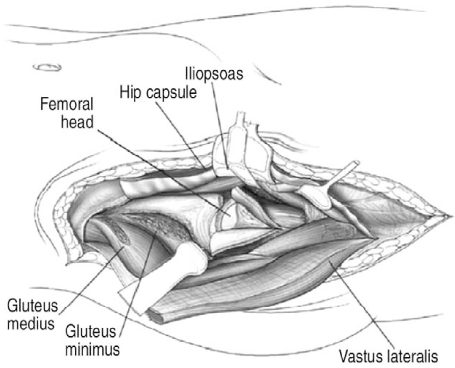
Fig. 4 Anterior approach: Deep dissection. Rectus femoris tendon has been released near its origin to allow further exposure of the medial hip capsule. In the proximal wound, a portion of the gluteus medius and gluteus minimus has been released to improve the exposure of the superior hip capsule.
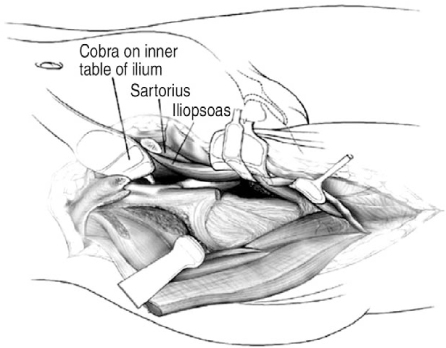
Fig. 5 Anterior approach: Extensive exposure. The exposure to the anterior column and medial acetabular wall can be accomplished by further dissection. The ASIS has been released and the sartorius and inguinal ligament retracted medially. The iliopsoas can be dissected posteriorly to expose a portion of the acetabular wall to the level of the sciatic notch.

Fig. 6 Anterolateral approach. The typical curvilinear incision for the anterolateral approach. For hip arthroplasty where greater exposure is needed, the apex of the incision may be placed more posterior to the level of the posterior edge of the greater trochanter. The fascial dissection is best started at the greater trochanter.
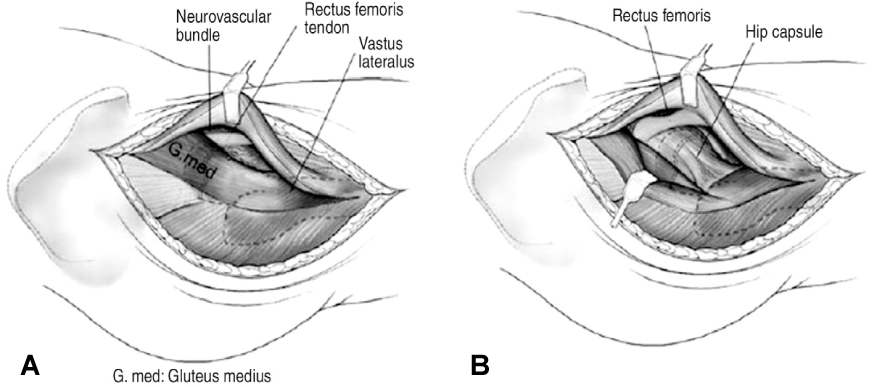
Fig. 7 Anterolateral approach: (A) The first branch is encountered a few centimeters proximal to the insertion of the gluteus medius. This connection is sacrificed to allow deeper exposure. (B) The minor vascular bundle is ligated between the tensor and the medius, but the proximal neurovascular bundle is preserved. The deep retraction of the gluteus medius posteriorly exposes the gluteus minimus tendon. Flexion and external rotation of the hip improves the exposure to the anterior hip capsule. The rectus still covers the anterior acetabular rim.
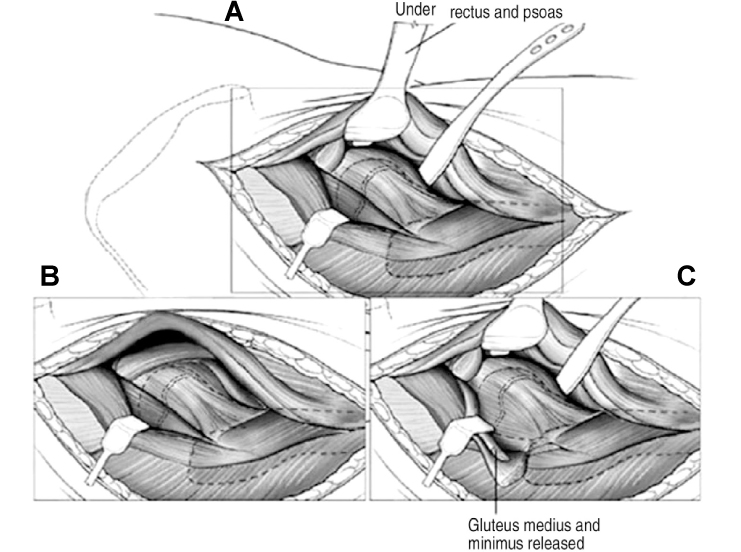
Fig. 8 Anterolateral approach: (A) For limited exposure of the hip, the rectus retractor may be placed above the rectus tendon. (B) The blunt rectus retractor is placed beneath the tendon and inside the pelvis to complete the medial exposure. A blunt inferior cobra retractor protects the vascular structures inferior to the hip capsule. (C) Improvement in the exposure of the superior capsule is obtained by the partial release of the gluteus medius and minimus from the anterior trochanter.
Reference
-
1. Moon DH. Anterior approach of the hip. J Korean Hip Soc. 2007. 19:319–323.2. Hardinge K. The direct lateral approach to the hip. J Bone Joint Surg Br. 1982. 64:17–19.
Article3. Smith-Petersen MN. Approach to and exposure of the hip joint for mold arthroplasty. J Bone Joint Surg Am. 1949. 31A:40–46.
Article4. Callaghan JJ, Rosenberg AG, Rubash HE. The adult hip. 2007. 2nd ed. Philadelphia: Lippincott Williams & Wilkins;685–694.5. Hoppenfeld S, deBoer P. Surgical exposure in orthopaedics. 2003. 3rd ed. Philadelphia: Lippincott Williams & Wilkins;365–453.6. Barton C, Kim PR. Complications of the direct anterior approach for total hip arthroplasty. Orthop Clin North Am. 2009. 40:371–375.
Article7. van Oldenrijk J, Hoogland PV, Tuijthof GJ, Corveleijn R, Noordenbos TW, Schafroth MU. Soft tissue damage after minimally invasive THA. Acta Orthop. 2010. 81:696–702.
Article8. Ivins GK. Meralgia paresthetica, the elusive diagnosis: clinical experience with 14 adult patients. Ann Surg. 2000. 232:281–286.9. Hueter C. Hueter C, editor. Fünfte abtheilung: die verletzung und krankheiten des hüftgelenkes, neunundzwanzigstes capitel. 1883. Leipzig: FCW Vogel;129–200.10. Ince A, Kemper M, Waschke J, Hendrich C. Minimally invasive anterolateral approach to the hip: risk to the superior gluteal nerve. Acta Orthop. 2007. 78:86–89.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Bernese Periacetabular Osteotomy Using Dual Approaches for Hip Dysplasias
- Patient Accompanied with Simultaneous Anterior Dislocation of Hip and Anterior Dislocation of Knee : A Case Report
- Prevention of Venous Thromboembolism in Hip Surgery Patients
- Treatment of Complex Tibial Plateau Fractures: A Modified Patient Positioning for the Combined Anterior and Posterior Approaches
- Bilateral Traumatic Anterior Dislocation of the Hips: A Case Report
