Comparison of Proximal Fusion to T1 or T2 in Double Thoracic Adolescent Idiopathic Scoliosis
- Affiliations
-
- 1Seoul Spine Institute, College of Medicine, Inje University, Sanggye Paik Hospital, Seoul, Korea. toetotoe1@sanggyepaik.ac.kr
- KMID: 2186557
- DOI: http://doi.org/10.4055/jkoa.2007.42.3.332
Abstract
-
PURPOSE: To assess the results of double thoracic fusion using pedicle screw instrumentation fused proximally to T1 or T2 in patients with double thoracic adolescent idiopathic scoliosis (AIS).
MATERIALS AND METHODS
Forty patients with double thoracic AIS were analyzed retrospectively after a minimum follow-up of 2 years. The patients were divided into two groups according to the proximal fusion level: the T1 group (n=26) was fused to T1 and the T2 group (n=14) was fused to T2.
RESULTS
There were no significant differences in the preoperative curve characteristics between the two groups. In the T1 group, the preoperative upper curve magnitude of 38+/-7o and apical vertebral translation (AVT) of 8+/-6 mm were corrected to 17+/-7o (54% correction) and 4+/-3 mm (3 mm correction) at the final follow-up, respectively. In the T2 group, the preoperative upper curve magnitude of 37+/-5o and the AVT of 7+/-4 mm were corrected to 22+/-6o (42% correction) and 6+/-3 mm (1 mm correction) at the final follow-up, respectively. There was no difference in the correction of lower thoracic curve, sagittal alignment and balance between the two groups. There was a significantly better correction in the upper thoracic curve and T1 tilting in the T1 group than the the T2 group.
CONCLUSION
In double thoracic AIS, fusions to T1 and T2 produce satisfactory results. However, fusion to T1 is recommended for a better correction of the upper curve and T1 tilting.
Figure
-
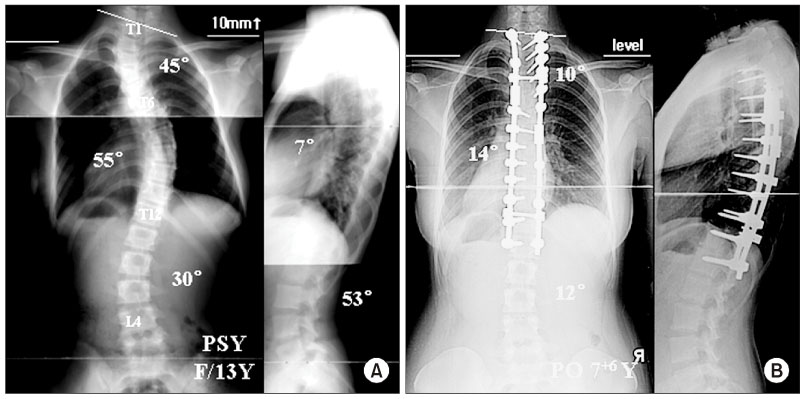
Fig. 1 (A) A 13-year-old girl with a double thoracic curve. She had an upper thoracic curve of 45°, lower thoracic curve of 55° and lumbar curve of 30°. T1 tilting of 15° and a shoulder height difference of 10 mm with the right shoulder elevated. (B) She was treated with double thoracic fusion using pedicle screw instrumentation from T1 to L1. Seven years and 6 months after surgery, the upper thoracic curve was corrected to 10°, the lower thoracic curve was corrected to 14° and lumbar curve was corrected to 12°. The T1 tilting was improved to 3° and the shoulders were level.
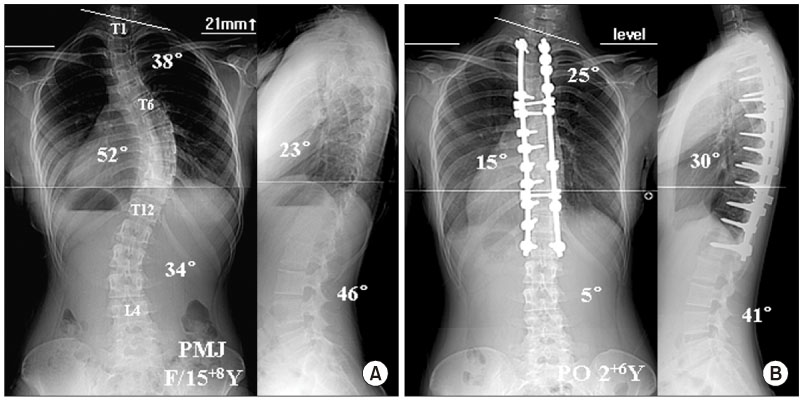
Fig. 2 (A) A 15-year-8-month-old girl with a double thoracic curve. She had an upper thoracic curve of 38°, a lower thoracic curve of 52° and a lumbar curve of 34°. T1 tilting was 10° and the shoulder height difference was 21 mm with the right shoulder elevated. (B) She was treated with the double thoracic fusion using pedicle screw instrumentation from T2 to L1. Two years and 6 months after surgery, the upper thoracic curve was corrected to 25°, the lower thoracic curve to 15° and the lumbar curve to 5°. The T1 tilt was aggravated to 16° and the shoulders were level.
Reference
-
1. Ginsburg H, Goldstein L, De Vanny J, Haake P. An evaluation of the upper thoracic curve in idiopathic scoliosis: guidelines in selection of the fusion area. Presented at the Annual Meeting of the Scoliosis Research Society. 1977. Hong Kong.2. King HA, Moe JH, Bradford DS, Winter RB. The selection of fusion levels in thoracic idiopathic scoliosis. J Bone Joint Surg Am. 1983. 65:1302–1313.
Article3. Lee CK, Denis F, Winter RB, Lonstein JE. Analysis of the upper thoracic curve in surgically treated idiopathic scoliosis: a new concept of the double thoracic curve pattern. Spine. 1993. 18:1599–1608.4. Lee DH, Lee JC, Kim SH, et al. Tactics for surgical treatment of the double thoracic scoliosis: significance of T1 tilt, first rib elevation and correction ratio. J Kor Spine Surg. 2002. 9:106–114.5. Lenke LG, Bridwell KH, O'Brien MF, Baldus C, Blanke K. Recognition and treatment of the proximal thoracic curve in adolescent idiopathic scoliosis treated with Cotrel-Dubousset instrumentation. Spine. 1994. 19:1589–1597.
Article6. Margulies JY, Floman Y, Robin GC, et al. An algorithm for selection of istumentation levels in scoliosis. Eur Spine J. 1998. 7:88–94.7. Moe JH, Kettleson DN. Idiopathic scoliosis An analysis of curve patterns and the preliminary results of Milwaukee brace treatment in 169 patients. J Bone Joint Surg Am. 1970. 52:1509–1533.8. Ponseti IV, Friedman B. Prognosis in idiopathic scoliosis. J Bone Joint Surg Am. 1950. 32:381–395.
Article9. Suk SI, Kim WJ, Lee CS, et al. Indication of proximal thoracic curve fusion in thoracic adolescent idiopathic scoliosis: recognition and treatment of double thoracic curve pattern in adolescent idiopathic scoliosis treated with segmental instrumentation. Spine. 2000. 25:2342–2349.10. Suk SI, Lee CK, Kim WJ, Chung YJ, Park YB. Segmental pedicle screw fixation in the treatment of thoracic idiopathic scoliosis. Spine. 1995. 20:1399–1405.
Article11. Suk SI, Lee CK, Min HJ, Cho KH, Oh JH. Comparison of Cotrel-Dubosset pedicle screws and hooks in the treatment of idiopathic scoliosis. Int Orthop. 1994. 18:341–346.
Article12. Winter RB. The idiopathic double thoracic curve pattern: its recognition and surgical management. Spine. 1989. 14:1287–1292.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Indications of Proximal Thoracic Curve Fusion in Thoracic Adolescent Idiopathic Scoliosis(AIS): Recognition and Treatment of Double Thoracic Curve Pattern in Adolescent Idiopathic Scoliosis Treated with Segmental Instrumentation
- Sagittal Plane Lumbar Responses after Anterior Selective Thoracic Fusion for Main Thoracic Adolescent Idiopathic Scoliosis
- The Efficacy of Proximal Lumbar Curve Flexibility in Patients with Main Thoracic Adolescent Idiopathic Scoliosis Treated by Selective Thoracic Fusion Surgery
- Tactics for Surgical Treatment of the Double Thoracic Scoliosis: Significance of T1 tilt, first rib elevation and correction ratio
- Clinical Results of Selective Thoracic Fusion by Segmental Pedicle Screws in King type II Adolescent Idiopathic Scoliosis ( AIS )
