Treatment of Bone Loss using Ilizarov Fixation after Resection ofBenign Tumor in the Long Bone
- Affiliations
-
- 1Department of Orthopaedic Surgery, Chonnam National University Hospital, Gwangju, Korea. madkid@dreamwiz.com
- KMID: 2186503
- DOI: http://doi.org/10.4055/jkoa.2007.42.4.426
Abstract
-
PURPOSE: This study analyzed the results of treatment of bone loss using Ilizarov fixation after resection of benign tumor in the long bone radiologically and clinically.
MATERIALS AND METHODS
Initial diagnoses were 5 osteofibrous dysplasia, 1 aneurysmal bone cyst and 1 giant cell tumor. Three indices were used to evaluate the results; percentage transport, healing index and percentage increase. The function of the affected limb was assessed according to Ennecking rating. And we assessed the radiological and functional results according to A.S.A.M.I.'s classification.
RESULTS
Percentage transport averaged 75% (range: 29-144), healing index averaged 64.5 day/cm (range: 34.8-108.6) and the percentage increase averaged 13% (range: 11-20). In Enneking rating, there were 6 cases that were classified as being better than good. In A.S.A.M.I.'s classification, there were 6 good cases, and 1 fair case each in the bone result and functional result, respectively.
CONCLUSION
Ilizarov technique is a reconstruction method using living bone. It is safe and effective for the treatment of bone loss after the resection of a benign tumor in the long bone.
Keyword
Figure
-

Fig. 1 (A) Radiographs of a 12-year-old male patient show an osteolytic lesion of left tibial shaft. (B) Coronal and sagittal images of computed tomograph show the same lesions. (C) We performed resection of the lesion and applied Ilizarov fixator. Pathologic diagnosis was osteofibrous dysplasia. (D) Radiographs of at 5 months postoperative show nonunion of docking site. (E) We performed a fibular strut bone graft at docking site. (F) Radiographs from the last follow-up show a healed bone lesion.
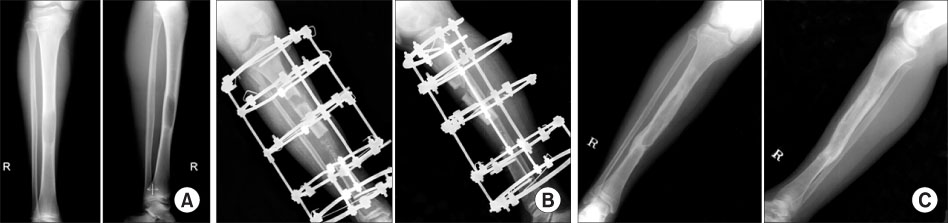
Fig. 2 (A) Radiographs of a 14-year-old male patient show an osteolytic lesion of the shaft of the right tibia. (B) We resected the lesion and inserted calcium sulfate into the bone defect and applied Ilizarov fixator. We simutaneously performed corticotomy at the proximal metaphysis. Radiographs at 1 month postoperative showed that the proximal fragment was transported distally. (C) Radiographs from the last follow-up show healed bone lesion.

Fig. 3 (A) Radiographs of a 15-year-old female patient show a pathologic fracture of the right distal femur. (B) We performed resecting of the lesion and applied Ilizarov fixator. (C) Radiographs at 2 months postoperative show lengthening of the corticotomy site. (D) Radiographs from the last follow-up show a healed bone lesion.
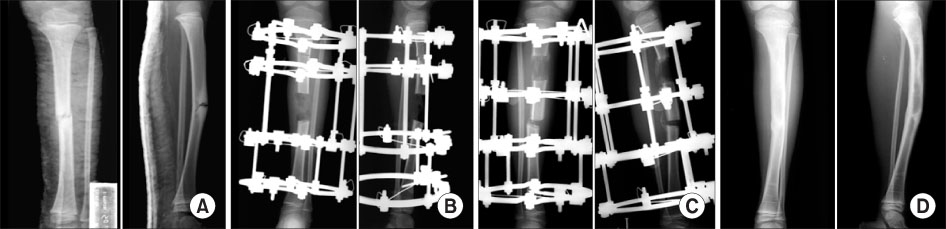
Fig. 4 (A) The image shows the pathologic fracture due to fibrous dysplasia of the diaphysis. (B) We resected the lesion and applied Ilizarov fixator. (C) We performed gradual lengthening at the proximal metaphysis. (D) Radiographs at the last follow-up show a healed bone lesion.
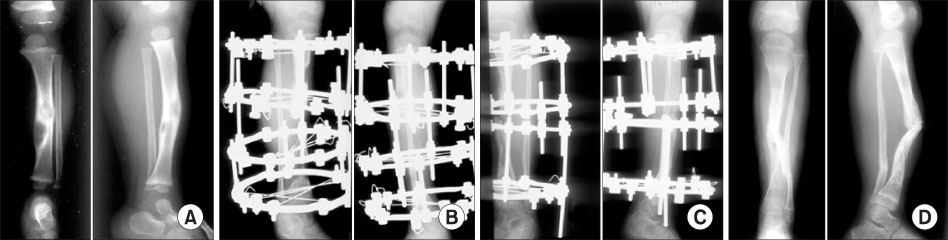
Fig. 5 (A) Radiographs of a 4-year-old male patient show an osteolytic lesion of the right tibial diaphysis. (B) We performed resecting of the lesion and applied Ilizarov fixator. (C) Radiographs at 12 months postoperative show lengthening of the corticotomy site. (D) Radiographs at the last follow-up show a healed bone lesion.
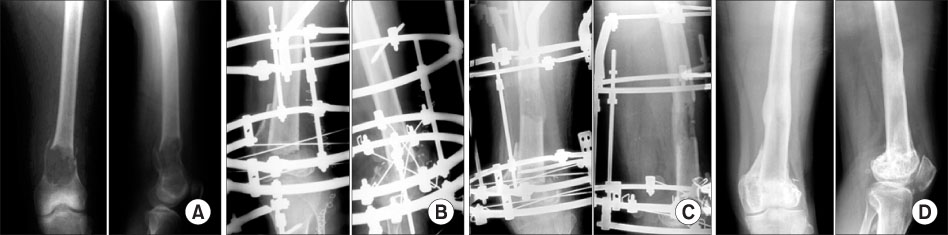
Fig. 6 (A) Radiographs of a 36-year-old male patient show an osteolytic lesion of the left dital femur. (B) We resected the lesion and applied Ilizarov fixator. (C) Radiographs at 9 months postoperative show lengthening of the corticotomy site. (D) Radiographs at 2 years postoperative show a healed bone lesion.

Fig. 7 (A) Radiographs of a 10-year-old male patient show an osteolytic lesion of the shaft of the right tibia. (B) We resected the lesion and inserted calcium sulfate and a fibular strut bone graft at the bone defect. (C) The image shows union processing at the graft site. (D) Radiographs at the last follow-up show a healed bone lesion.
Reference
-
1. Abbott LC. The operative lengthening of the tibia and fibula. J Bone Joint Surg. 1927. 9:128.
Article2. Anderson WV. Leg-lengthening, in proceedings of the British Orthopedic Association. J Bone Joint Surg Br. 1952. 34:150.3. Cierny G 3rd, Zorn KE. Segmental tibial defects. Comparing conventional and Ilizarov methodologies. Clin Orthop Relat Res. 1994. 301:118–123.4. Codivillar A. On the means of lengthening, in the lower limbs, the muscles and tissues which are shortened through deformity. 1904. Clin Orthop Relat Res. 1994. 301:4–9.5. Enneking WF. Ennecking WF, editor. A system for functional evaluation of the surgical management of musculoskeletal tumors. Limb salvage in musculoskeletal oncology. 1987. New York: Churchill Livingstone;5–16.6. Hahn SB, Park EH, Park HW, Kim HW, Kim BH. Comparison of treating tibial nonunion with bone and soft tissue defect: Ilizarov only versus free flap and Ilizarov. J Korean Orthop Assoc. 2002. 37:754–758.
Article7. Ilizarov GA. The tension-stress effect on the genesis and growth of tissue: Part II. The influence of the rate and frequency of distraction. Clin Orthop Relat Res. 1989. 239:263–285.8. Ilizarov GA. Clinical application of tension-stress effect for limb lengthening. Clin Orthop Relat Res. 1990. 250:8–26.9. Karita M, Tsuchiya H, Sakurakichi K, Tomita K. Osteofibrous dysplasia treated with distraction osteogenesis: a report of two cases. J Orthop Sci. 2004. 9:516–520.
Article10. Lee DY, Choi IH, Chung CY, Lee KH, Kim HS. Our experience on leg lengthening by the Ilizarov technique. -A preliminary report on the first seventeen patients-. J Korean Orthop Assoc. 1990. 25:1611–1623.
Article11. Paley D, Catagni MA, Argnani F, Villa A, Benedetti GB, Cattaneo R. Ilizarov treatment of tibial nonunions with bone loss. Clin Orthop Relat Res. 1989. 241:146–165.
Article12. Paley D, Fleming B, Pope M, Kristansen T. A comparative study of fracture gap motion and shear in external fixation. Presented at the Conference on Recent Advances in External Fixation. Riva Del Garda. 1986. 28–30.13. Song HR, Cho SH, Koo KH, et al. Treatment of tibial bone defect by internal bone transport using Ilizarov method. J Korean Orthop Assoc. 1996. 31:1071–1079.
Article14. Subasi M, Kapukaya A. Distraction osteogenesis for treatment of bone loss in the lower extremity. J Orthop Sci. 2003. 8:882–884.
Article15. Tsuchiya H, Tomita K. Distraction osteogenesis for treatment of bone loss in the lower extremity. J Orthop Sci. 2003. 8:116–124.
Article16. Tsuchiya H, Tomita K, Shinokawa Y, Minematsu K, Katsuo S, Taki J. The Ilizarov method in the management of giant-cell tumours of the proximal tibia. J Bone Joint Surg Br. 1996. 78:264–269.
Article17. Tsuchiya H, Tomita K, Minematsu K, Mori Y, Asada N, Kitano S. Limb salvage using distraction osteogensis. A classification of the technique. J Bone Joint Surg Br. 1997. 79:403–411.18. Vassershtein IS. Distraction-compression method of elongation of the lower extremity with use of bone tubular homotransplant. Orthop Travmatol Protez. 1968. 29:44–48.19. Wagner H. Operative lengthening of the femur. Clin Orthop Relat Res. 1978. 136:125–142.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of the Difficult Fractures of the Femur using the Ilizarov External Fixator
- Ilizarov External Fixation for the Complications of Supracondylar Fracture of Femur: Report of two cases
- Bone Transport for Reconstruction in Benign Bone Tumors
- The Treatment of Infected Nonunions of the Tibia by the Methods of Ilizarov
- External Fixation of Long Bone Fractures in Children
