Chondrosarcoma of the Pelvis following Internal Pelvectomy:Functional and Oncological Results
- Affiliations
-
- 1Department of Orthopedic Surgery, Korea Cancer Center Hospital, Seoul, Korea. dgjeon@kcch.re.kr
- KMID: 2186502
- DOI: http://doi.org/10.4055/jkoa.2007.42.4.417
Abstract
-
PURPOSE: We analyzed the nature of primary chondrosarcoma of the pelvis, along with long-term survival, complications, and functional outcomes.
MATERIALS AND METHODS
Twenty-five cases of pelvic chondrosarcoma were enrolled. The average age was 40 (range: 17-69) years. The stage was IB in 5, IIB in 20. All of the 25 cases had underwent internal pelvectomy. Twelve cases had resections involving the acetabulum, while 7 involved the iliac wing and 6 involved the pubic bone. Study points were the reconstructive methods according to the extent of resection and the functional results, complications, local recurrence and the metastasis pattern following the clinical factors affecting long-term survival.
RESULTS
The 16-year CDF survival of 25 cases following operation was 78.7%. Three (12%) local recurrences and 3 metastases occurred. The MSTS score of the iliac and pubic resection group was 25.3. Of 12 cases with acetabular resection, 6 had prosthetic arthroplasty, 4 had psuedoarthrosis, 1 had arthrodesis, and 1 had excision. Their overall MSTS score was 19.4. There were 2 infections, 1 flap necrosis, 1 screw failure and 2 hip dislocations. Of 11 cases of a high grade (G3), there were 3 metastases and 1 local recurrence.
CONCLUSION
The long-term survival rate was good and the pathologic grade had some correlation with prognosis. Because acetabular reconstructions of any kind may involve serious complications, primary pseudoarthrosis can be regarded as an alternative option.
MeSH Terms
Figure
-
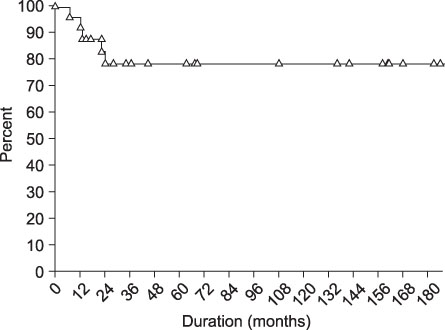
Fig. 1 Long-term survival of 25 cases following operation.
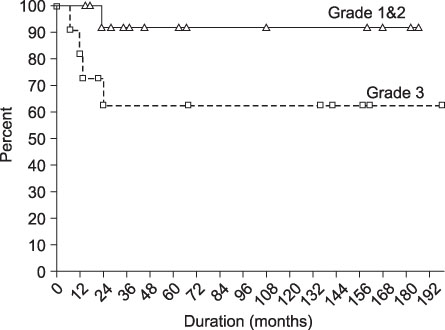
Fig. 2 Cumulative survival according to pathologic grade (p= 0.05).

Fig. 3 (A) Plain radiograph shows the minimal osteolytic region on the acetabular dome area of the left ilium. (B) On the T1W1 MRI image, low signal lesion can be observed on the acetabulum. (C) Type II resection and reconstruction was performed with a saddle-type tumor prosthesis. (D, E) Plain radiograph and T2WI MRI show a huge calcified mass in the left inguinal area suggesting recurrence at 6 months postoperatively.

Fig. 4 (A) Plain radiograph and MRI shows calcified mass extending from the superior ramus to the inner pelvic cavity. (B) Type I+II+III resection and reconstruction were performed with THRA-heat treated autogenous bone composite. (C) The heat-treated bone and hardware were removed 10 days after the operation due to infection. Seven years later, pseudoarthrosis was complete with shortening of the affected limb.

Fig. 5 (A) Plain X-ray shows a huge calcified mass extending from the pubic ramus to the adductor group. (B) CT scan shows a huge mass arising from the pubic bone with some abutment to the lesser trochanter. (C) Type II+III resection and reconstruction were performed with a saddle-type tumor prosthesis. (D) Four years postoperatively, dislocation of the implant occurred due to screw failure, and open reduction ensued.

Fig. 6 (A) Plain radiograph shows a sclerotic lesion in the right ilium and sacro-iliac joint. (B) The T2WI MRI shows a huge mass extending from the right iliac fossa extending to the pelvic cavity. (C) Type I resection was performed, followed by a strut bone graft from the contralateral iliac cortex. (D) Thirteen years postoperatively, internal rotation of the remaining segment, sclerotic changes of the symphysis pubis, and some shortening were evident. However, the patient had no problems performing daily activities.
Reference
-
1. Aboulafia AJ, Buch R, Mathews J, Li W, Malawer MM. Reconstruction using the saddle prosthesis following excision of primary and metastatic periacetabular tumors. Clin Orthop Relat Res. 1995. 314:203–213.
Article2. Aboulafia AJ, Malawer MM. Surgical management of pelvic and extremity of osteosarcoma. Cancer. 1993. 71:Suppl 10. 3358–3366.3. Bell RS, Davis AM, Wunder JS, Buconjic T, McGoveran B, Gross AE. Allograft reconstruction of the acetabulum after resection of stage-IIB sarcoma. Intermediate-term results. J Bone Joint Surg Am. 1997. 79:1663–1674.4. Björnsson J, McLeod RA, Unni KK, Ilstrup DM, Pritchard DJ. Primary chondrosarcoma of long bones and limb girdles. Cancer. 1998. 83:2105–2119.
Article5. Enneking WF, Dunham WK. Resection and reconstruction for primary neoplasms involving the innominate bone. J Bone Joint Surg Am. 1978. 60:731–746.
Article6. Enneking WF, Dunham W, Gebhardt MC, Malawer M, Pritchard DJ. A system for the functional evaluation of reconstructive procedures after surgical treatment of tumors of the musculoskeletal system. Clin Orthop Relat Res. 1993. 286:241–246.
Article7. Enneking WF, Spanier SS, Goodman MA. A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop Relat Res. 1980. 153:106–120.
Article8. Evans HL, Ayala AG, Romsdahl MM. Prognostic factors in chondrosarcoma of bone: a clinicopathologic analysis with emphasis on histologic grading. Cancer. 1977. 40:818–831.9. Harrington KD. The use of hemipelvic allografts or autoclaved grafts for reconstruction after wide resections of malignant tumors of the pelvis. J Bone Joint Surg Am. 1992. 74:331–341.
Article10. Healey JH, Lane JM. Chondrosarcoma. Clin Orthop Relat Res. 1986. 119–129.11. Johnson S, Têtu B, Ayala AG, Chawla SP. Chondrosarcoma with an additional mesenchymal component (dedifferentiated chondrosarcoma). I. A clinicopathologic study of 26 cases. Cancer. 1986. 58:278–286.12. Lee FY, Mankin HJ, Fondren G, et al. Chondrosarcoma of bone: an assessment of outcome. J Bone Joint Surg Am. 1999. 81:326–338.13. Lichtenstein L, Jaffe HL. Chondrosarcoma of bone. J Pathol. 1943. 19-A:553–589.14. Marcove RC, Mike V, Hutter RV, et al. Chondrosarcoma of the pelvis and the upper end of the femur. An analysis of factors influencing survival time in one hundred and thirteen cases. J Bone Joint Surg Am. 1972. 54:561–572.15. O'Connor MI, Sim FH. Salvage of the limb in the treatment of malignant pelvic tumors. J Bone Joint Surg Am. 1989. 71:481–494.16. Ozaki T, Hillmann A, Lindner N, Blasius S, Winkelmann W. Chondrosarcoma of the pelvis. Clin Orthop Realt Res. 1997. 226–239.
Article17. Pring ME, Weber KL, Unni KK, Sim FH. Chondrosarcoma of the pelvis. A review of sixty-four cases. J Bone Joint Surg Am. 2001. 83:1630–1642.18. Pritchard DJ, Lunke RJ, Taylor WF, Dahlin DC, Medley BE. Chondrosarcoma: a clinico-pathologic and statistical analysis. Cancer. 1980. 45:149–157.
Article19. Sheth DS, Yasko AW, Johnson ME, Ayala AG, Murray JA, Romsdahl MM. Chondrosarcoma of the pelvis. Prognostic factors for 67 patients treated with definitive surgery. Cancer. 1996. 78:745–750.
Article20. Shives TC, McLeod RA, Unni KK, Schray MF. Chondrosarcoma of the spine. J Bone Joint Surg Am. 1989. 71:1158–1165.
Article21. Stephenson RB, Kaufer H, Hankin FM. Partial pelvic resection as an alternative to hindquarter amputation for skeletal neoplasms. Clin Orthop Relat Res. 1989. 242:201–211.
Article22. Uchida A, Myoul A, Araki N, Yoshikawa H, Ueda T, Aoki Y. Prosthetic reconstruction for periacetabular malignant tumors. Clin Orthop Relat Res. 1996. 326:238–245.
Article23. Windhager R, Karner J, Kutschera HP, Polterauer P, Salzer-Kuntschik M, Kotz R. Limb salvage in periacetabular sarcomas: review of 21 consecutive cases. Clin Orthop Relat Res. 1996. 331:265–276.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical and Oncological Outcome of Pelvis Bone Tumor Patients with Type III Internal Hemipelvectomy
- Chondrosarcoma of the Pelvis
- Long-term Outcome of Chondrosarcoma: A Single Institutional Experience
- Oncologic and Functional Outcomes of Extended Curettage for Low-Grade Central Chondrosarcoma
- Chondrosarcoma in Pelvis
