Change of Deformity due to Position and Anesthesia in Adolescent Idiopathic Scoliosis
- Affiliations
-
- 1Department of Orthopaedic Surgery, Asan Medical Center College of Medicine, University of Ulsan, Seoul, Korea. cslee@amc.seoul.kr
- 2Department of Orthopaedic Surgery, National Police Hospital, Seoul, Korea.
- KMID: 2186449
- DOI: http://doi.org/10.4055/jkoa.2008.43.3.329
Abstract
-
PURPOSE: To determine changes in the end vertebra and neutral vertebra as well as in the magnitudes of coronal and rotational deformities according to position and anesthesia in patients with adolescent idiopathic scoliosis.
MATERIALS AND METHODS
Sixty-two structural curves in 31 patients were evaluated using standing, supine, side bending, post-anesthesia, and postoperative anteroposterior plain radiographs. Cobb angles and rotation angles by perdriolle torsionmeter were measured, and the end vertebra and neutral vertebra were identified in each radiograph.
RESULTS
Coronal cobb angles decreased significantly with correction rates of 25.0%, 31.7%, 59.5%, and 74.0%, and rotational deformities decreased with correction ratesof 6.1%, 24.5%, 6.2%, and 25.7% by supine position, anesthesia, side bending and surgery, respectively.The end vertebrae changed in 18 patients (58.1%) in both supine and post-anesthesia radiographs, and the neutral vertebrae changed in 10 patients (32.3%) in supine radiographs and in 20 patients (64.5%) in post-anesthesia radiographs.
CONCLUSION
Coronal deformities are significantly corrected by supine position and anesthesia. Anesthesia significantly corrects axial rotation, but more correction cannot be achieved by rod derotation. The end vertebra and neutral vertebra have a tendency to vary by position and anesthesia, which gives rise to confusion in the determination of fusion level.
Keyword
Figure
-
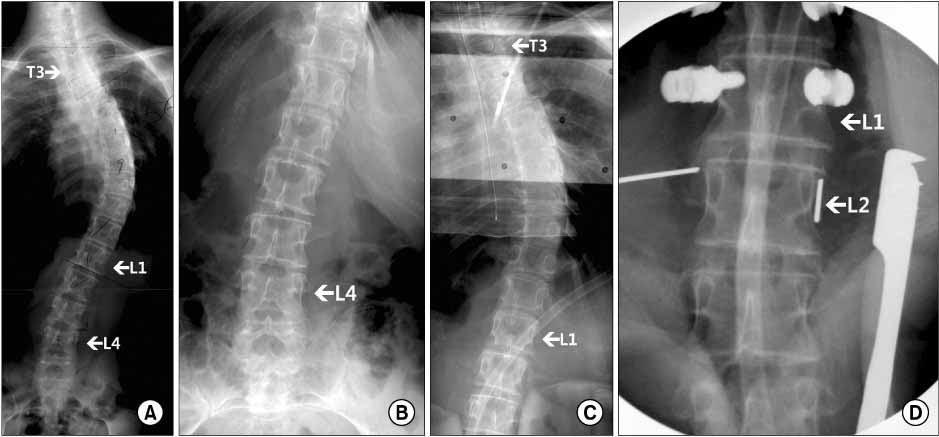
Fig. 1 Preoperative whole spine anteroposterior standing (A), lumbar spine supine (B), post-anesthesia (C) radiographs and an image taken by C-arm fluoroscopy during an L2 screw insertion (D) of a 18-year old female patient with adolescent idiopathic scoliosis (Case 23). In a standing radiograph, the end vertebrae of the curve were identified as T5 and L1, and the neutral vertebrae were T3 and L5. The lower end vertebra, however, changed to T12 in a post-anesthesia radiograph. The neutral vertebrae were so variable that the pedicle shadows of L4 were not symmetric in a standing radiograph, but became so in the supine one. Moreover, T4 and L1 were neutral in post-anesthesia film, and the image on the C-arm clearly demonstrates that vertebral rotation is converted to the opposite direction between L1 and L2. The angles of rotation at which symmetric pedicle images could be obtained by C-arm image intensifier in L1 and L2 were counterclockwise 3 degrees and clockwise 5 degrees, respectively.
Reference
-
1. Behairy YM, Hauser DL, Hill D, Mahood J, Moreau M. Partial correction of cobb angle prior to posterior spinal instrumentation. Ann Saudi Med. 2000. 20:398–401.
Article2. Cheung KM, Luk KD. Prediction of correction of scoliosis with use of the fulcrum bending radiograph. J Bone Joint Surg Am. 1997. 79:1144–1150.
Article3. Chi JH, Lee R, Mummaneni PV. Concepts of surgical correction-segmental derotation and translation techniques. Neurosurg Clin N Am. 2007. 18:325–328.
Article4. Cobb JR. Outline for the study of scoliosis. Am Acad Orthop Surg Instruc Lect. 1948. 5:261–275.5. Davis BJ, Gadgil A, Trivedi J, Ahmed el-NB. Traction radiography performed under general anesthetic: a new technique for assessing idiopathic scoliosis curves. Spine. 2004. 29:2466–2470.
Article6. Delorme S, Labelle H, Poitras B, Rivard CH, Coillard C, Dansereau J. Pre-, intra-, and postoperative three-dimensional evaluation of adolescent idiopathic scoliosis. J Spinal Disord. 2000. 13:93–101.
Article7. Duke K, Aubin CE, Dansereau J, Labelle H. Biomechanical simulations of scoliotic spine correction due to prone position and anesthesia prior to surgical instrumentation. Clin Biomech (Bristol, Avon). 2005. 20:923–931.8. Gstoettner M, Sekyra K, Walochnik N, Winter P, Wachter R, Bach CM. Inter-and intraobserver reliability assessment of the Cobb angle: manual versus digital measurement tools. Eur Spine J. 2007. 16:1587–1592.9. King HA, Moe JH, Bradford DS, Winter RB. The selection of fusion levels in thoracic idiopathic scoliosis. J Bone Joint Surg Am. 1983. 65:1302–1313.
Article10. Klepps SJ, Lenke LG, Bridwell KH, Bassett GS, Whorton J. Prospective comparison of flexibility radiographs in adolescent idiopathic scoliosis. Spine. 2001. 26:E74–E79.
Article11. Labelle H, Dansereau J, Bellefleur C, de Guise J, Rivard CH, Poitras B. Perioperative three-dimensional correction of idiopathic scoliosis with the Cotrel-Dubousset procedure. Spine. 1995. 20:1406–1409.12. Lee CS, Kim MJ, Ahn YJ, Kim YT, Jeong KI, Lee DH. Thoracic pedicle screw insertion in scoliosis using posteroanterior C-arm rotation method. J Spinal Disord Tech. 2007. 20:66–71.
Article13. Lee SM, Suk SI, Chung ER. Direct vertebral rotation: a new technique of three-dimensional deformity correction with segmental pedicle screw fixation in adolescent idiopathic scoliosis. Spine. 2004. 29:343–349.
Article14. Lenke LG, Betz RR, Harms J, et al. Adolescent idiopathic scoliosis: a new classification to determine extent of spinal arthrodesis. J Bone Joint Surg Am. 2001. 83:1169–1181.15. Omeroğlu H, Ozekin O, Bicimoğlu A. Measurement of vertebral rotation in idiopathic scoliosis using the perdriolle torsionmeter: a clinical study on intraobserver and interobserver error. Eur Spine J. 1996. 5:167–171.
Article16. Perdriolle R, Vidal J. Thoracic idiopathic scoliosis curve evolution and prognosis. Spine. 1985. 10:785–791.
Article17. Polly DW Jr, Sturm PF. Traction versus supine side bending: which technique best determines curve flexibility? Spine. 1998. 23:804–808.18. Potter BK, Rosner MK, Lehman RA Jr, Polly DW Jr, Schroeder TM, Kuklo TR. Reliability of end, neutral, and stable vertebrae identification in adolescent idiopathic scoliosis. Spine. 2005. 30:1658–1663.
Article19. Shah SA. Derotation of the spine. Neurosurg Clin N Am. 2007. 18:339–345.
Article20. Shea KG, Stevens PM, Nelson M, Smith JT, Masters KS, Yandow S. A comparison of manual versus computer-assisted radiographic measurement. Intraobserver measurement variability for Cobb angles. Spine. 1998. 23:551–555.21. Suk SI, Lee CK, Kim WJ, Chung YJ, Park YB. Segmental pedicle screw fixation in the treatment of thoracic idiopathic scoliosis. Spine. 1995. 20:1399–1405.
Article22. Suk SI, Lee SM, Chung ER, Kim JH, Kim WJ, Sohn HM. Determination of distal fusion level with segmental pedicle screw fixation in single thoracic idiopathic scoliosis. Spine. 2003. 28:484–491.
Article23. Torell G, Nachemson A, Haderspeck-Grib K, Schultz A. Standing and supine cobb measures in girls with idiopathic scoliosis. Spine. 1985. 10:425–427.
Article24. Vedantam R, Lenke LG, Bridwell KH, Linville DL. Comparison of push-prone and lateral-bending radiographs for predicting postoperative coronal alignment in thoracolumbar and lumbar scoliotic curves. Spine. 2000. 25:76–81.
Article25. Yazici M, Acaroglu ER, Alanay A, Deviren V, Cila A, Surat A. Measurement of vertebral rotation in standing versus supine position in adolescent idiopathic scoliosis. J Pediatr Orthop. 2001. 21:252–256.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Correction in Rotational Deformity with Thoracolumbosacral Orthosis in Idiopathic Scoliosis
- Spontaneous Rib Fracture during Boston Brace Treatment for Adolescent Idiopathic Scoliosis
- Relation of Radiographic Parameters and Psychosocial Condition in Idiopathic Adolescent Scoliosis
- Letter to the Editor: Optimizing deformity correction: a retrospective comparative analysis of two techniques in high-magnitude curves in adolescent idiopathic scoliosis
- Etiology of Adolescent Idiopathic Scoliosis: A Literature Review
