The Treatment of Infected Nonunions of Femur using Sequestrectomy and Distraction Osteogenesis
- Affiliations
-
- 1Department of Orthopaedic Surgery, Chonnam National University Hospital, Gwangju, Korea. stjung@chonnam.ac.kr
- KMID: 2186423
- DOI: http://doi.org/10.4055/jkoa.2008.43.5.610
Abstract
-
PURPOSE: From this study we are to know the result of distraction osteogenesis for infected nonunions of femur using sequestrectomy and Ilizarov external fixator.
MATERIALS AND METHODS
17 patients who had distraction osteogenesis using external fixator and also had more than 2.5 cm bone loss after sequestrectomy for having infected nonunions of femur from 1991 to 2005. Their average age was 32.4 (range, 10-60) years and mean follow up period was 22 (range, 14-36) months. We used Healing index as an index for bone formation. The results were divided into bone results and functional results and analyzed by grading. Also we estimated the complication according to the Paley's classification.
RESULTS
After seqestrectomy, bone defect was ranged from 5cm to 13 cm (average, 7.3 cm) and The average of transportation was 5.8 cm (range, 3-10 cm). HI was 47.4 (27.17-65.80) days/cm. Solid bony union occurred in the all cases after surgery but, 4 cases needed bone graft at docking site. According to the final examination there were 2 cases with leg-length discrepancy that is bigger than 2.5 cm and the average size of was 1.0 cm.
CONCLUSION
We consider distraction osteogenesis using Ilizarov external fixator as useful method to restore bone loss caused after sequestrectomy for infected nonunions of femur.
Keyword
MeSH Terms
Figure
-
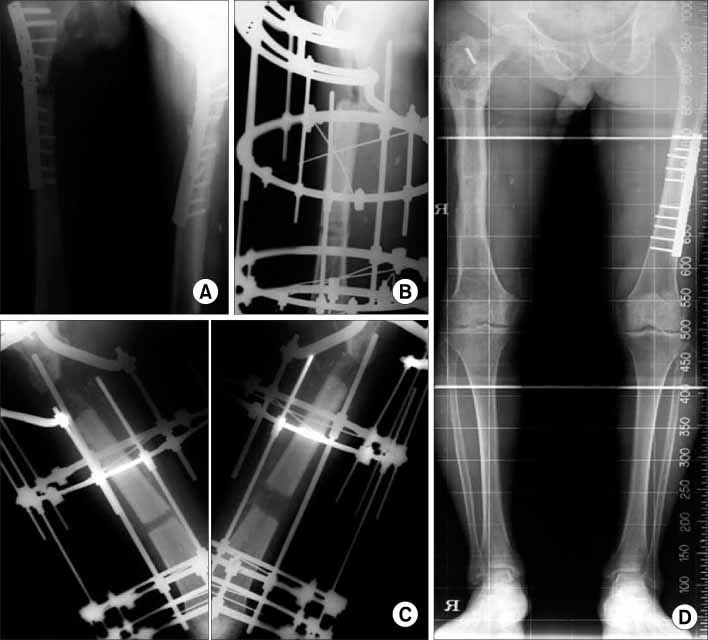
Fig. 1 (A) A 54 years male had the open type IIIa fracture at proximal femur shaft. He underwent a surgery using plates by internal fixation. (B) We did sequestrectomy, applied ilizarov fixator and corticotomy at the distal femur. (C) We did gradual bone transportation. (D) At last follow-up, the final discrepancy of leg length was 1.5 centimeters.
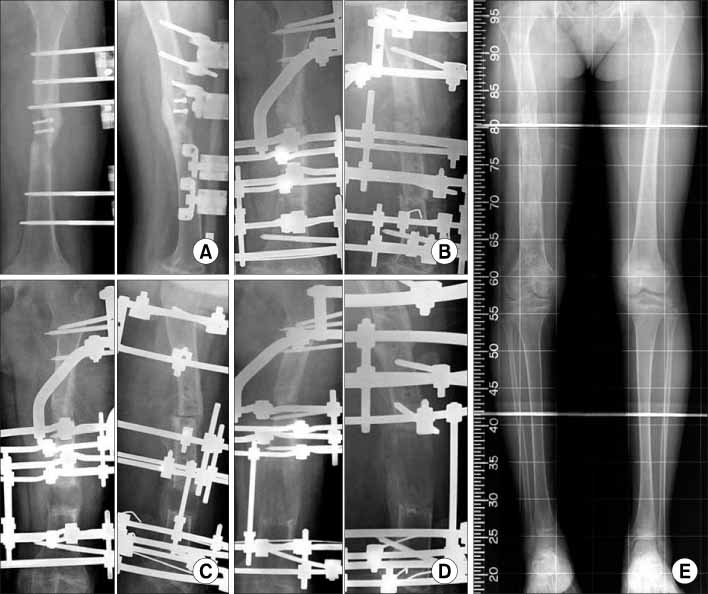
Fig. 2 (A) A 10 years male had the type IIIa open femur shaft fracture and underwent a surgery using mono-external fixator, (B) After five months later, he underwent a revision surgery with ilizarov and an infectious segment resection. There was a bone defect about 5 centimeters. We made acute docking of a resected segment and did corticotomy at the distal femur. (C, D) Distraction about 5 centimeters was done and the EF time was 6.8 months. (E) At final follow-up, there was no leg length discrepancy.
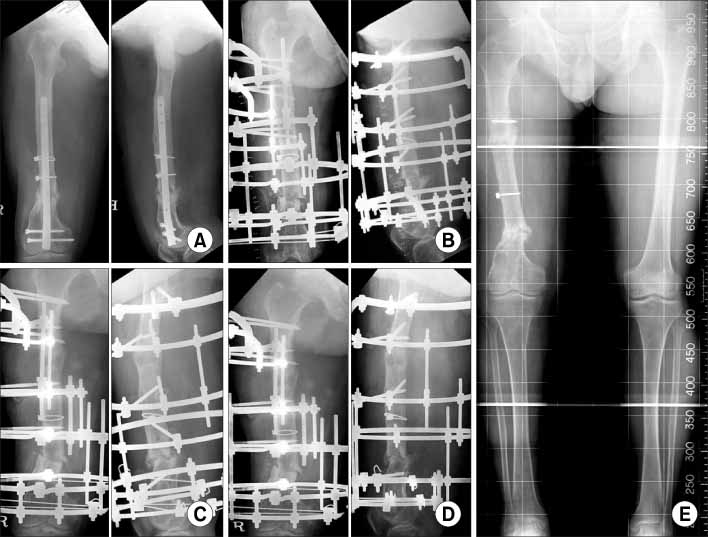
Fig. 3 (A) A 51-years male was sustained open communited fracture of the right femur by a traffic accident. Interlocking intramedullary nailing was done at a local clinic but developed an infected nonunion. (B) We did sequestrectomy, applied ilizarov fixatior and did corticotomy after implants removal. We did gradual bone transfortation. (C) Four months later, radiographs after ilizarov fixation didn't show the evidence of union on the distal femur. (D) We did bone graft on a delayed union site. (E) Follow up 3 months, X-ray after bone graft on a sequestrectomy site was showed a complete bony union.
Reference
-
1. Aldegheri R. Femoral callotasis. J Pediatr Orthop. 1997. 6:42–47.
Article2. Aronson J. Temporal and spatial increases in blood flow during distraction osteogenesis. Clin Orthop Relat Res. 1994. 301:124–131.
Article3. Cattaneo R, Catagni M, Johhson EE. The treatment of infected nonunions and segmental defects of the tibia by the methods of Ilizarov. Clin Orthop Relat Res. 1992. 280:143–152.
Article4. Cierny G, Madar JT. Everts CM, editor. Classification and treatment of adult osteomyelitis. Surgery of the musculosketal system. 1990. New York, NY: Churdhill Livingstone;4337.5. Dendrinos GK, Kontos S, Lyritsis E. Use of the Ilizarov technique for treatment of nonunion of the tibia associated with infection. J Bone Joint Surg Am. 1995. 77:835–846.
Article6. De Bastiani G, Aldegheri R, Renzi-Brivio L, Trviella G. Limb lengthening by callus distraction (callotasis). J Pediat Orthop. 1987. 7:129–134.7. Dendrinos GK, Kontos S, Lyritsis E. Use of the Ilizarov technique for treatment of non-union of the tibia associated with infection. J Bone Joint Surg Am. 1995. 77:835–846.
Article8. Glorion C, Pouliquen JC, Langlais J, Ceolin JL, Kassis B. Femoral lengthening using the callotasis method: study of the complications in a series of 70 cases in children and adolescents. J Pediatr Orthop. 1996. 16:161–167.
Article9. Green SA. Osteomyelitis. The Ilizarov perspective. Orthop Clin North Am. 1991. 2:515–521.10. Green SA, Dlabal TA. The open bone graft for septic nonunion. Clin Orthop Relat Res. 1983. 180:117–124.
Article11. Ilizarov GA. The tension-stress effect on the genesis and growth of tissues: Part II. The influence of stability of fixation and soft-tissue perservation. Clin Orthop Relat Res. 1989. 239:263–285.12. Kabata T, Tsuchiya H, Sakurakichi K, Yamashiro T, Watanabe K, Tomita K. Reconstruction with distraction osteogenesis for juxta-articular nonunions with bone loss. J Trauma. 2005. 58:1213–1222.
Article13. Kapukaya A, Subasi M, Kandiya E, Ozates M, Yilmaz F. Limb reconstruction with the callus distraction method after bone tumor resection. Arch Orthop Trauma Surg. 2000. 120:215–218.
Article14. Marsh DR, Shah S, Elliot J, Kurdy N. The Ilizarov method in non-union, malunion and infection of fractures. J Bone Joint Surg Br. 1997. 79:273–279.
Article15. May JW, Jupiter JB, Weiland AJ, Byrd HS. Clinical classification of post-traumatic tibial osteomyelitis. J Bone Joint Surg Am. 1989. 71:1422. Current Concepts Review.
Article16. Minematsu K, Tsuchiya H, Taki J, Tomita K. Blood flow measurement during distraction osteogenesis. Clin Orthop Relat Res. 1998. 347:229–235.
Article17. Paley D. Problems, obstacles, and complications of limb lengthening by the Ilzarov technique. Clin Orthop Relat Res. 1990. 250:81–104.18. Paley D, Catagni MA, Argnani F, Villa A, Bennedetti GB, Cattaneo R. Iiazrov treatment of tibial nonunions with bone loss. Clin Orthop Relat Res. 1989. 241:146–165.19. Saridis A, Panagiotopoulos E, Tyllianakis M, Matzaroglou C, Vandoros N, Lambiris E. The use of the Ilizarov method as a salvage procedure in infected nonunion of the distal femur with bone loss. J Bone Joint Surg Br. 2005. 88:232–237.
Article20. Tsuchiya H, Tomita K, Minematsu K, Mori Y, Asada N, Kitano S. Limb salvage using distraction osteogenesis. A classification of the technique. J Bone Joint Surg Br. 1997. 79:403–411.21. Ueng SW, Chuang CC, Cheng SL, Shih CH. Management of large infected tibial defects with radical dibridement and staged double-rib composite free transfer. J Trauma. 1996. 40:345–350.22. Ueng SW, Wei FC, Shih CH. Management of large infected tibial defects with antibiotic beads local therapy and staged fibular osteoseptocutaneous free transfer. J Trauma. 1997. 43:268–274.
Article23. Ueng SW, Wei FC, Shih CH. Management of femoral diaphyseal infected nonunion with antibiotic beads local therapy, external skeletal fixation, and staged bone grafting. J Trauma. 1999. 46:97–103.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of Infected Nonunion of the Femur with Marked Shortening by Compression and Gradual Distraction at the Nonunion Site: A Report of 2 cases
- Case reports of antero-posteior movement with distraction osteogenesis in maxillary anterior segment
- Distraction osteogenesis in facial asymmetry patient
- Serial Change of the Bone Density in Distraction Osteogenesis in Long Bone Lengthening in Lower Extremity - by the Pixel Value in PACS
- The effect of oscillating distraction osteogenesis on new bone formation during mandibular distraction period in rabbits
