Outcome Analysis of Single Level Anterior Cervical Fusion using Interbody PEEK Cage with Autologous Iliac Bone Graft
- Affiliations
-
- 1Department of Orthopedic Surgery, School of Medicine, Kyung Hee University, Seoul, Korea. skd111@khmc.or.kr
- KMID: 2186383
- DOI: http://doi.org/10.4055/jkoa.2009.44.1.93
Abstract
- PURPOSE
Anterior cervical fusion with a tricortical iliac bone graft is a well established procedure for treating degenerative cervical spine disease. An interbody cage has been used to prevent donor site morbidity but there are few reports on the clinical and radiological outcome.
MATERIALS AND METHODS
Thirty eight patients, who underwent single level ACDF with PEEK interbody Solis(R)cage (Stryker spine, South Allendale, NJ, USA), were enrolled in this study. This study evaluated Odom's criteria and visual analogue scale (VAS) for the neck, arm and donor site pain, and the radiological findings, including the disk height, cage subsidence, and sagittal alignment of cervical spine.
RESULTS
The mean disk height loss was 1.1 mm during the follow up period. Case subsidence >2 mm developed in 17 cases (44.7%). The mean subsidence of this group was 3.09 mm. The bone union rate was 95% at 12 weeks. There was no significant change in the sagittal alignment of the cervical spine. The VAS for neck, arm, and donor site pain improved all cases. Only 9 patients complained of mild discomfort at the donor site
CONCLUSION
Single-level ACDF using PEEK interbody cage has a lack of donor site morbidity, excellent clinical outcomes and bone union. However, more study of the factors related to postoperative cage subsidence will be needed.
Keyword
MeSH Terms
Figure
-
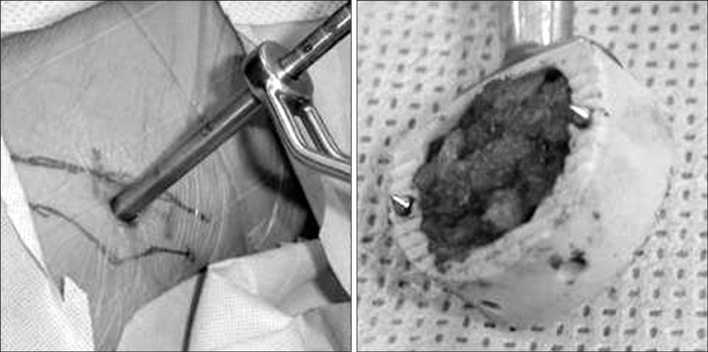
Fig. 1 Photographs showing havesting technique of autologous bone with minimal incision at anterior iliac crest and PEEK cage (Solis®, Stryker spine) filled with cancellous bone.

Fig. 2 Lateral radiograph of cervical spine showing disc height measuring method. Disc height=A+M+P 3.
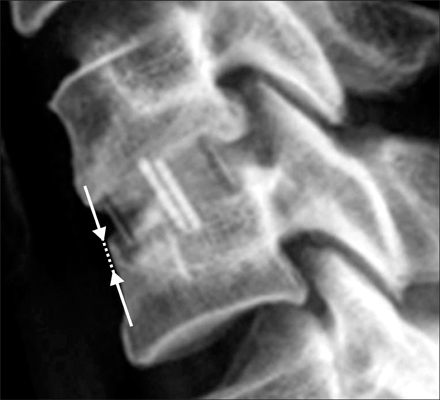
Fig. 3 Lateral radiograph of cervical spine showing cage subsidence measurement.

Fig. 4 Lateral radiograph of cervical spine showing segmental height measuring method.
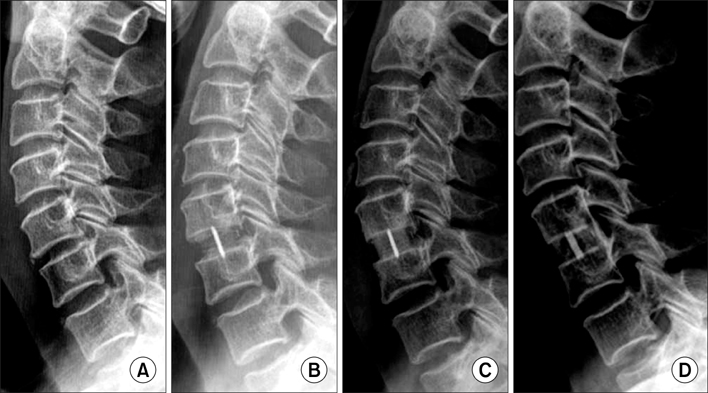
Fig. 5 Serial radiographs of 64-year-old female patient underwent C5/6 anterior cervical fusion using stand alone PEEK cage. Preoperative (A) and immediate postoperative radiograph (B) show increased disc height in C5/6. Follow radiographs showing solid union without subsidence at 3 months (C) and 36 months after operation.
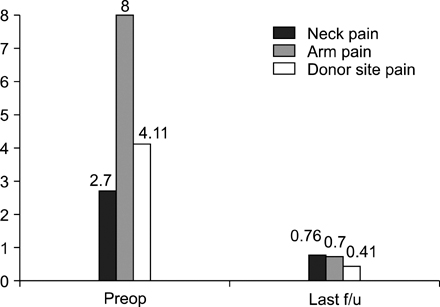
Fig. 6 Graph showing the clinical outcome analysis with VAS for neck, arm and donor site pain.

Fig. 7 Graph showing the change of mean disk height.
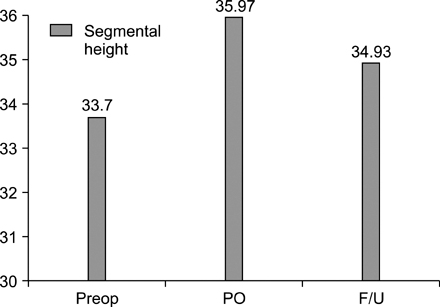
Fig. 8 Graph showing the change of mean segmental height.
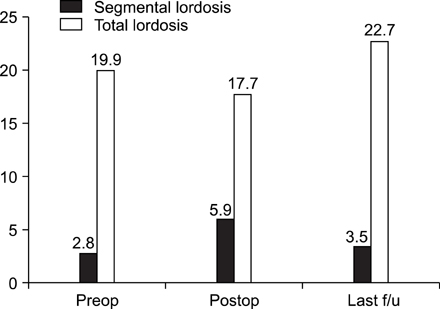
Fig. 9 Graph showing the change of sagittal alignment of cervical spine.
Cited by 3 articles
-
Subsidence and Nonunion after Anterior Cervical Interbody Fusion Using a Stand-Alone Polyetheretherketone (PEEK) Cage
Jae Jun Yang, Chang Hun Yu, Bong-Soon Chang, Jin Sup Yeom, Jae Hyup Lee, Choon-Ki Lee
Clin Orthop Surg. 2011;3(1):16-23. doi: 10.4055/cios.2011.3.1.16.Efficacy of PEEK Cages and Plate Augmentation in Three-Level Anterior Cervical Fusion of Elderly Patients
Kyung Jin Song, Gyu Hyung Kim, Byeong Yeol Choi
Clin Orthop Surg. 2011;3(1):9-15. doi: 10.4055/cios.2011.3.1.9.Anterior Cervical Fusion Using a Zero-Profile Stand-Alone Cage: Radiological and Clinical Outcomes after More than 2 Years of Follow-Up
Han Chang, Byung-Wan Choi
J Korean Soc Spine Surg. 2016;23(3):146-153. doi: 10.4184/jkss.2016.23.3.146.
Reference
-
1. Abd-Alrahman N, Dokmak AS, Abou-Madawi A. Anterior cervical discectomy (ACD) versus anterior cervical fusion (ACF). Clinical and radiological outcome study. Acta Neurochir (Wien). 1999. 141:1089–1092.
Article2. An HS, Simpson JM, Glover JM, Stephany J. Comparison between allograft plus demineralized bone matrix versus autograft in anterior cervical fusion. A prospective multicenter study. Spine. 1995. 20:2211–2216.3. Bagby GW. Arthrodesis by the distraction-compression method using a stainless steel implant. Orthopedics. 1988. 11:931–934.
Article4. Bartels RH, Donk RD, Feuth T. Subsidence of stand-alone cervical carbon fiber cages. Neurosurgery. 2006. 58:502–508.
Article5. Bishop RC, Moore KA, Hadley MN. Anterior cervical interbody fusion using autogenic and allogenic bone graft substrate: a prospective comparative analysis. J Neurosurg. 1996. 85:206–210.6. Cauthen JC, Kinard RE, Vogler JB, et al. Outcome analysis of noninstrumented anterior cervical discectomy and interbody fusion in 348 patients. Spine. 1998. 23:188–192.
Article7. Cauthen JC, Theis RP, Allen AT. Anterior cervical fusion: a comparison of cage, dowel and dowel-plate constructs. Spine J. 2003. 3:106–117.8. Cho D, Liau W, Lee W, Lin JT, Chin CL, Shen PC. Preliminary experience using a polyetherertherketone (PEEK) cage in the treatment of cervical disc disease. Neurosurgery. 2002. 51:1343–1350.9. Ciccone WJ 2nd, Motz C, Bentley C, Tasto JP. Bioabsorbable implants in orthopaedics: new developments and clinical applications. J Am Acad Orthop Surg. 2001. 9:280–288.
Article10. Cloward RB. The anterior approach for removal of ruptured cervical disks. J Neurosurg. 1958. 15:602–617.
Article11. Coric D, Branch CL Jr, Jenkins JD. Revision of anterior cervical pseudoarthrosis with anterior allograft fusion and plating. J Neurosurg. 1997. 86:969–974.12. DeBowes RM, Grant BD, Bagby GW, Gallina AM, Sande RD, Ratzlaff MH. Cervical vertebral interbody fusion in the horse: a comparative study of bovine xenografts and autografts supported by stainless steel baskets. Am J Vet Res. 1984. 45:191–199.13. Geisler F, Caspar W, Pitzen T, Johnson TA. Reoperation in patients after anterior cervical plate stabilization in degenerative disease. Spine. 1998. 23:911–920.
Article14. Gercek E, Arlet V, Delisle J, Marchest D. Subsidence of stand-alone cervical cages in anterior interbody fusion: warning. Eur Spine J. 2003. 12:513–516.
Article15. Goh JC, Wong HK, Thambyah A, Yu CS. Influence of PLIF cage size on lumbar spine stability. Spine. 2000. 25:35–39.
Article16. Hacker R, Cauthen JC, Gilbert TJ, Griffith SL. A prospective randomized multicenter clinical evaluation of an anterior cervical fusion cage. Spine. 2000. 25:2646–2655.
Article17. Kulkarni AG, Hee HT, Wong HK. Solis cage (PEEK. for anterior cervical fusion: preliminary radiological results with emphasis on fusion and subsidence. Spine J. 2007. 7:205–209.
Article18. Löfgren H, Johannsson V, Olsson T, Ryd L, Levander B. Rigid fusion after Cloward operation for cervical disc disease using autograft allograft, or xenograft: a randomized study with radiostereometic and clinical follow-up assessment. Spine. 2000. 25:1908–1916.19. López-Olivia Muñoz F, Garcia de las Heras B, Concejero López V, Asenjo Siguero JJ. Comparison of three techniques of anterior fusion in single-level cervical disc herniation. Eur Spine J. 1998. 7:512–516.20. Lowery G, McDonough RF. The significance of hardware failure in anterior cervical plate fixation. Patients with 2- to 7-year follow-up. Spine. 1998. 15:181–186.21. Majd ME, Vadhva M, Holt RT. Anterior cervical reconstruction using titanium cages with anterior plating. Spine. 1999. 24:1604–1610.
Article22. Savolainen S, Rinne J, Hernesniemi J. A prospective randomized study of anterior single-level cervical disc operations with long-term follow-up: surgical fusion is unnecessary. Neurosurgery. 1998. 43:51–55.
Article23. Sawain PD, Traynelis VC, Menezes AH. A comparative analysis of fusion rates and donor-site morbidity for autogeneic rib and iliac crest bone grafts in posterior cervical fusions. J Neurosurg. 1998. 88:255–265.24. Schmieder K, Schönmayr R, Goetz C, et al. Kaech DL, Jinkins JR, editors. Anterior cervical interbody fusion with Wing titanium cages. Spinal restabilization procedures. diagnostic and therapeutic aspects of intervertebral fusion cages, artificial discs and mobile implants. 2002. Boston: Elsevier;229–234.25. Shapiro S. Banked fibula and the locking anterior cervical plate in anterior cervical fusions following cervical discectomy. J Neurosurg. 1996. 84:161–165.
Article26. Smith GW, Robinson RA. Treatment of certain cervical spine disorders by anterior removal of the intervertebral disc and interbody fusion. J Bone Joint Surg Am. 1958. 40:607–624.27. Tribus C, Corteen DP, Zdeblick TA. The efficacy of anterior cervical plating in the management of symptomatic pseudoarthrosis of the cervical spine. Spine. 1999. 24:860–864.
Article28. Truumees E, Demetropoulos CK, Yang KH, Herkowitz HN. Effects of a cervical compression plate on graft forces in an anterior cervical discectomy model. Spine. 2003. 28:1097–1102.
Article29. van Jonbergen HP, Spruit M, Anderson PG, Pavlov PW. Anterior cervical interbody fusion with a titanium box cage: early radiological assessment of fusion and subsidence. Spine J. 2005. 5:645–649.
Article30. Wang JC, McDonough PW, Endow KK, Delamarter RB. Increased fusion rates with cervical plating for two-level anterior cervical discectomy and fusion. Spine. 2000. 25:41–45.
Article31. Wilke HJ, Kettler A, Goetz C, Claes L. Subsidence resulting from simulated postoperative neck movements: an in vitro investigation with a new cervical fusion cage. Spine. 2000. 25:2762–2770.32. Zaveri GR, Ford M. Cervical spondylosis: the role of anterior instrumentation after decompression and fusion. J Spinal Disord. 2001. 14:10–16.
Article33. Zoega B, Kärrholm J, Lind B. Plate fixation adds stablity to two-level anterior fusion in the cervical spine: a randomized study using radiostereometry. Eur Spine J. 1998. 7:302–307.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Usefulness of Anterior Cervical Interbody Fusion Using Locally Harvested Bone: Locally Harvested Bone Versus Autogenous Iliac Bone
- Efficiency of Anterior Interbody Fusion using Cage Packed with DBM in the Distractive Flexion Injury of Cervical Spine: Demineralized Bone Matrix vs Autoiliac Cancellous Bone
- Clinical Results from Subsidence and Loss of Lordosis after Anterior Cervical Discectomy and Fusion
- Polyetheretherketone Cage with Demineralized Bone Matrix Can Replace Iliac Crest Autografts for Anterior Cervical Discectomy and Fusion in Subaxial Cervical Spine Injuries
- The Availability of Autogenous Bicortical Iliac Bone Graft in Anterior Cervical Interbody Fusion
