J Korean Orthop Assoc.
2009 Jun;44(3):395-400. 10.4055/jkoa.2009.44.3.395.
Restless Legs Syndrome Mimicking Lower Leg Pain of Spinal Origin :Report on Two Cases
- Affiliations
-
- 1Department of Orthopaedic Surgery, School of Medicine, Wonkwang University Hospital, Iksan, Korea. osktg@wonkwang.ac.kr
- KMID: 2186350
- DOI: http://doi.org/10.4055/jkoa.2009.44.3.395
Abstract
- Restless legs syndrome (RLS) is a neurogenic disorder with the patients having a sensation of discomfort and an urge to move continuously. These symptoms can get worse during night and cause sleep disturbance. These symptoms can be misdiagnosed as lower leg pain of a spinal origin and the treatment can be wrongly focused on this. This treatment for an unproven state of symptoms can place clinicians in a difficult situation. We experienced RLS associated with spondylolisthesis and spinal stenosis, and we originally misdiagnosed the patient and wrongly treated the patient operatively with spinal fusion and posterior instrumentation. After an insufficient result, we diagnosed the patient with having RLS with the help of the neurology department and rehabilitation medical department. In one other case we diagnosed a RLS patient with the help of a neurologist and the patients had arrived an our department for total knee arthroplasty and spinal root block. We report on these cases so other orthopedic surgeons will not make same mistakes.
Keyword
MeSH Terms
Figure
-
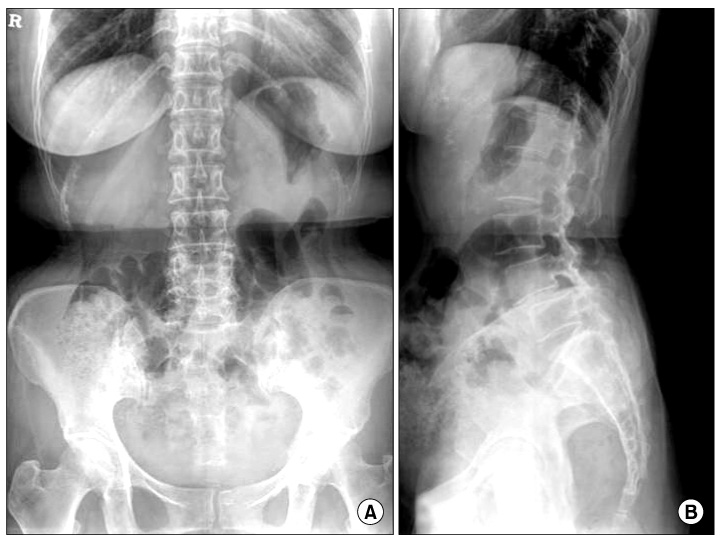
Fig. 1 Preoperative radiographs of the lumbar spine. Lateral radiograph showing spondylolisthesis at L4/5.
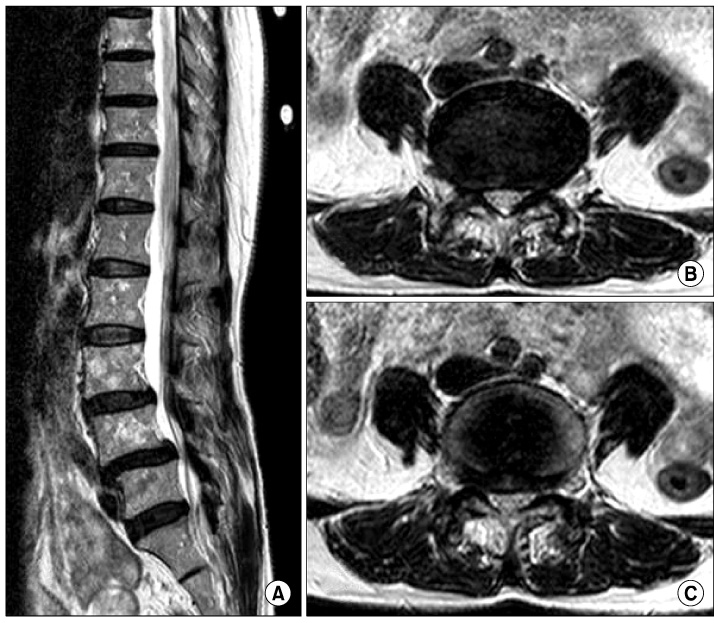
Fig. 2 Preoperative MRI imaging. MRI showed spinal stenosis at L4/5. B, L4/5; C, L4/5.
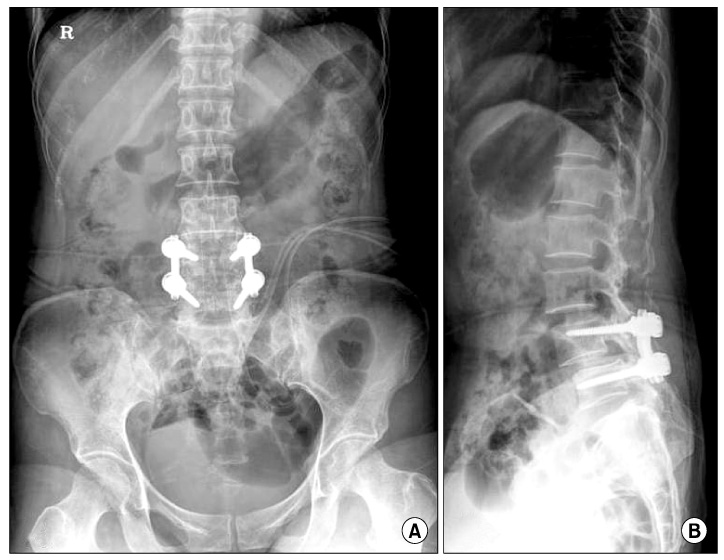
Fig. 3 Postoperative radiographs of the lumbar spine. Plane lumbar spine radiographs shows pedicle screw stabilization on L4/5.

Fig. 4 Radiograph of the right knee. Radiograph shows arthritic change of the knee.
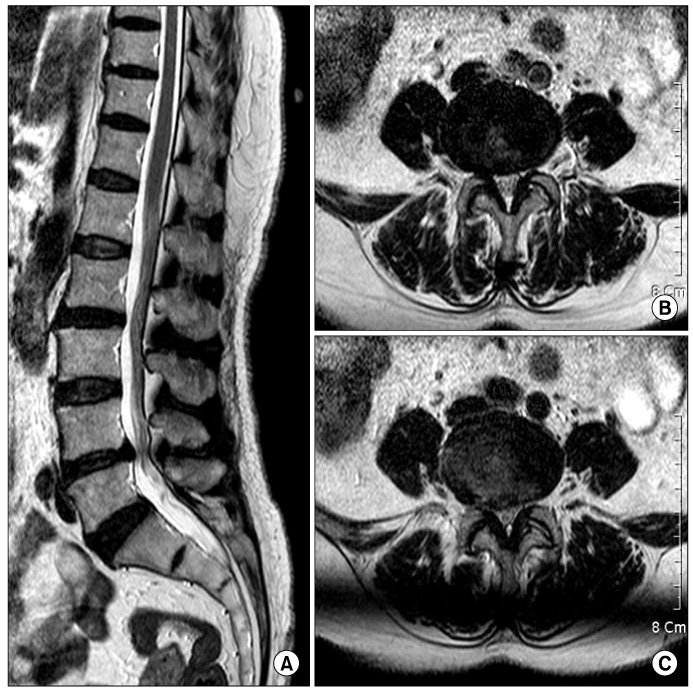
Fig. 5 MRI imaging. MRI showed spinal stenosis at L4/5.
Reference
-
1. Cho YW, Shin WC, Yun CH, et al. Epidemiology of restless legs syndrome in Korean adults. Sleep. 2008. 31:219–223.
Article2. Ekbom K. Restless legs syndrome. Acta Med Scand. 1945. 158:4–124.3. Hening W, Allen R, Earley C, Kushida C, Picchietti D, Silber M. The treatment of restless legs syndrome and periodic limb movement disorder. An American Academy of Sleep Medicine Review. Sleep. 1999. 22:970–999.4. Hening W, Walters AS, Allen RP, Montplaisir J, Myers A, Ferini-Strambi L. Impact, diagnosis and treatment of restless legs syndrome (RLS) in a primary care population: the REST (RLS epidemiology, symptoms, and treatment) primary care study. Sleep Med. 2004. 5:237–246.
Article5. Montplaisir J, Godbout R, Poirier G, Bedard MA. Restless legs syndrome and periodic movements in sleep: physiopathology and treatment with L-dopa. Clin Neuropharmacol. 1986. 9:456–463.6. Picchietti D, Winkelman JW. Restless legs syndrome, periodic limb movements in sleep, and depression. Sleep. 2005. 28:891–898.7. Stupar M. Restless legs syndrome in a primary contact setting: a case report. JCCA J Can Chiropr Assoc. 2008. 52:81–87.8. Trenkwalder C, Paulus W, Walters AS. The restless legs syndrome. Lancet Neurol. 2005. 4:465–475.
Article9. Yun CH. Pathophysiology of the restless legs syndrome: dopamine and iron. J Korean Sleep Soc. 2006. 3:22–28.
Article10. Zucconi M, Ferini-Strambi L. Epidemiology and clinical findings of restless legs syndrome. Sleep Med. 2004. 5:293–299.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Periodic Limb Movement and Restless legs Syndrome in Neurological Disorders
- Arm and Leg Restlessness After Acute Internal Capsular Infarction
- A Single Low Dose of Mirtazapine can Induce Restless Legs Syndrome: Report of Two Cases
- Effect of a Complex Leg Exercise Program for Hemodialysis Patients with Restless Legs Syndrome
- A Case of Restless Leg Syndrome Induced by Mirtazapine in a Patient with Major Depressive Disorder
