J Korean Orthop Assoc.
2014 Feb;49(1):43-49. 10.4055/jkoa.2014.49.1.43.
Correlation between Femoral Tunnel Location in Three-Dimensional Computed Tomography and Femoral Tunnel Angle in Plain Radiographs after Single-Bundle Anterior Cruciate Reconstruction
- Affiliations
-
- 1Department of Orthopedic Surgery, Chonbuk National University Hospital, Research Institute of Clinical Medicine, Chonbuk National University Medical School, Jeonju, Korea. hyukpark@jbnu.ac.kr
- KMID: 2185251
- DOI: http://doi.org/10.4055/jkoa.2014.49.1.43
Abstract
- PURPOSE
The purpose of this study is to determine correlation between femoral tunnel angle in the coronal plane on a simple radiograph and femoral tunnel location in the sagittal plane on three-dimensional computed tomography (3D-CT).
MATERIALS AND METHODS
The subjects included 42 patients who underwent 3D-CT after the operation out of 70 cases of anterior cruciate ligament reconstruction using quadriceps tendon-patelllar bone autograft from April, 2009 to June, 2011. Measurement of the femoral tunnel angle was based on the anatomical axis of the femur in antero-posterior (AP) and Rosenberg views; femoral tunnel location was described as a proportional percentage on the medial surface of the lateral femoral condyle in the 3D-CT image; then the correlation between femoral tunnel angle and femoral tunnel location was analyzed retrospectively.
RESULTS
Femoral tunnel angle was 41.5degrees+/-6.8degrees (range: 29.7degrees-53.9degrees) on AP radiographs, and 34.9degrees+/-6.9degrees (range: 23.8degrees-46.5degrees) on Rosenberg views. The femoral tunnel was located 36.9%+/-11.3% from posterior, and 38.1%+/-6.5% from proximal on the 3D-CT image. On plain AP radiographs, femoral tunnel angle and femoral tunnel location showed negative correlation (p<0.001, rho=-0.498), and, in comparison with Rosenberg view, they showed negative correlation (p=0.006, rho=-0.416). Twenty three patients (53.5%) had femoral tunnel in the anatomical location. Their femoral tunnel angle on AP radiographs was 43.3degrees+/-6.1degrees, while the femoral tunnel angle of patients who had femoral tunnel in non-anatomical locations was 38.4degrees+/-6.4degrees (p=0.004). In the Rosenberg picture, similar difference was observed between the two groups (p=0.012).
CONCLUSION
On AP radiographs and Rosenberg views, femoral tunnel angle showed significant correlation with the femoral tunnel location on the 3D-CT image, and the group who had femoral tunnel location in the anatomical range showed a relatively higher femoral tunnel angle.
Keyword
MeSH Terms
Figure
-
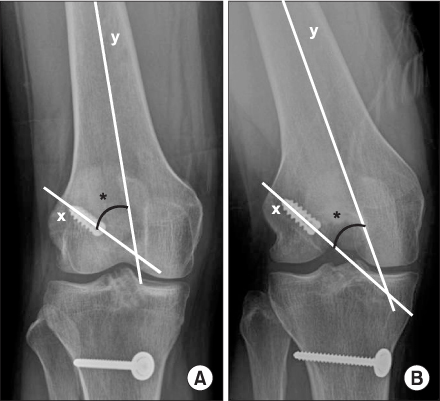
Figure 1 The femoral tunnel angle (*) is measured from the longitudinal axis of the femoral tunnel (x) and anatomical axis (y) of the femur on antero-posterior (A) and Rosenberg views (B).

Figure 2 Femoral tunnel location was described as a proportional percentage (from proximal to distal and posterior to anterior) on the medial surface of the lateral femoral condyle in the three-dimensional computed tomography image. The circle showed position of the graft in femoral tunnel.
Reference
-
1. Scopp JM, Jasper LE, Belkoff SM, Moorman CT 3rd. The effect of oblique femoral tunnel placement on rotational constraint of the knee reconstructed using patellar tendon autografts. Arthroscopy. 2004; 20:294–299.
Article2. Wetzlera MJ, Getelman MH, Friedman MJ, Bartolozzi AR. Revision anterior cruciate ligamentsurgery: etiology of failures. Oper Tech Sports Med. 1998; 6:64–70.3. Heming JF, Rand J, Steiner ME. Anatomical limitations of transtibial drilling in anterior cruciate ligament reconstruction. Am J Sports Med. 2007; 35:1708–1715.
Article4. Loh JC, Fukuda Y, Tsuda E, Steadman RJ, Fu FH, Woo SL. Knee stability and graft function following anterior cruciate ligament reconstruction: comparison between 11 o'clock and 10 o'clock femoral tunnel placement. 2002 Richard O'Connor Award paper. Arthroscopy. 2003; 19:297–304.5. Yagi M, Wong EK, Kanamori A, Debski RE, Fu FH, Woo SL. Biomechanical analysis of an anatomic anterior cruciate ligament reconstruction. Am J Sports Med. 2002; 30:660–666.
Article6. Forsythe B, Kopf S, Wong AK, et al. The location of femoral and tibial tunnels in anatomic double-bundle anterior cruciate ligament reconstruction analyzed by three-dimensional computed tomography models. J Bone Joint Surg Am. 2010; 92:1418–1426.
Article7. Kopf S, Forsythe B, Wong AK, et al. Nonanatomic tunnel position in traditional transtibial single-bundle anterior cruciate ligament reconstruction evaluated by three-dimensional computed tomography. J Bone Joint Surg Am. 2010; 92:1427–1431.
Article8. Lertwanich P, Martins CA, Asai S, Ingham SJ, Smolinski P, Fu FH. Anterior cruciate ligament tunnel position measurement reliability on 3-dimensional reconstructed computed tomography. Arthroscopy. 2011; 27:391–398.
Article9. Illingworth KD, Hensler D, Working ZM, Macalena JA, Tashman S, Fu FH. A simple evaluation of anterior cruciate ligament femoral tunnel position: the inclination angle and femoral tunnel angle. Am J Sports Med. 2011; 39:2611–2618.10. van Eck CF, Lesniak BP, Schreiber VM, Fu FH. Anatomic single- and double-bundle anterior cruciate ligament reconstruction flowchart. Arthroscopy. 2010; 26:258–268.
Article11. Woo SL, Kanamori A, Zeminski J, Yagi M, Papageorgiou C, Fu FH. The effectiveness of reconstruction of the anterior cruciate ligament with hamstrings and patellar tendon. A cadaveric study comparing anterior tibial and rotational loads. J Bone Joint Surg Am. 2002; 84:907–914.12. Bedi A, Musahl V, Steuber V, et al. Transtibial versus anteromedial portal reaming in anterior cruciate ligament reconstruction: an anatomic and biomechanical evaluation of surgical technique. Arthroscopy. 2011; 27:380–390.
Article13. Jepsen CF, Lundberg-Jensen AK, Faunoe P. Does the position of the femoral tunnel affect the laxity or clinical outcome of the anterior cruciate ligament-reconstructed knee? A clinical, prospective, randomized, double-blind study. Arthroscopy. 2007; 23:1326–1333.
Article14. Sadoghi P, Kröpfl A, Jansson V, Müller PE, Pietschmann MF, Fischmeister MF. Impact of tibial and femoral tunnel position on clinical results after anterior cruciate ligament reconstruction. Arthroscopy. 2011; 27:355–364.
Article15. Johnson DL, Swenson TM, Irrgang JJ, Fu FH, Harner CD. Revision anterior cruciate ligament surgery: experience from Pittsburgh. Clin Orthop Relat Res. 1996; 325:100–109.
Article16. Ristanis S, Giakas G, Papageorgiou CD, Moraiti T, Stergiou N, Georgoulis AD. The effects of anterior cruciate ligament reconstruction on tibial rotation during pivoting after descending stairs. Knee Surg Sports Traumatol Arthrosc. 2003; 11:360–365.
Article17. Bernard M, Hertel P, Hornung H, Cierpinski T. Femoral insertion of the ACL. Radiographic quadrant method. Am J Knee Surg. 1997; 10:14–21.18. Hoser C, Tecklenburg K, Kuenzel KH, Fink C. Postoperative evaluation of femoral tunnel position in ACL reconstruction: plain radiography versus computed tomography. Knee Surg Sports Traumatol Arthrosc. 2005; 13:256–262.
Article19. Pinczewski LA, Salmon LJ, Jackson WF, von Bormann RB, Haslam PG, Tashiro S. Radiological landmarks for placement of the tunnels in single-bundle reconstruction of the anterior cruciate ligament. J Bone Joint Surg Br. 2008; 90:172–179.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Correlation of Tunnel Position, Orientation and Tunnel Enlargement in Outside-in Single-Bundle Anterior Cruciate Ligament Reconstruction
- Three-Dimensional Reconstruction Computed Tomography Evaluation of the Tunnel Location and Angle in Anatomic Single-Bundle Anterior Cruciate Ligament Reconstruction: A Comparison of the Anteromedial Portal and Outside-in Techniques
- Evaluation of Femoral Tunnel Positioning Using 3-Dimensional Computed Tomography and Radiographs after Single Bundle Anterior Cruciate Ligament Reconstruction with Modified Transtibial Technique
- Tomographic Study of Femoral Positioning in Anterior Cruciate Ligament Reconstruction Using the Transtibial Technique
- Three-Dimensional Reconstruction Computed Tomography Evaluation of Tunnel Location during Single-Bundle Anterior Cruciate Ligament Reconstruction: A Comparison of Transtibial and 2-Incision Tibial Tunnel-Independent Techniques
