J Korean Orthop Assoc.
2014 Apr;49(2):133-139. 10.4055/jkoa.2014.49.2.133.
A Two-Stage Approach to Primary Total Knee Arthroplasty in Recurrent Septic Arthritis
- Affiliations
-
- 1Department of Orthopedic Surgery, Yeungnam University Medical Center, Daegu, Korea. ossoj@med.yu.ac.kr
- KMID: 2185218
- DOI: http://doi.org/10.4055/jkoa.2014.49.2.133
Abstract
- PURPOSE
The purpose of this study is to evaluate the usefulness of a two-stage approach to primary knee arthroplasty with recurrent septic arthritis.
MATERIALS AND METHODS
We studied 22 patients with recurrent septic arthritis, and we observed them for more than one year of follow-up survey from January 2005 to April 2012 at Yeungnam University Medical Center. The clinical assessment was performed following Knee Society knee score, Knee Society function score, and International Knee Documentation Committee Score (IKDC) subjective assessment. In addition, we analyzed the causative organisms, significant medical comorbidities (diabetes mellitus), period up to primary knee arthroplasty, and radiologic assessment with reference to disease prognosis.
RESULTS
The average range of postoperative knee motion showed a good result, with an average of 115degrees. Knee Society knee score improved from 23.5 to 81.0, and Knee Society function score also increased from 22.5 to 73.2. Subjective assessment by IKDC was divided into 15 normal patients and 7 nearly normal patients. No significant difference was observed between patients with causative organisms and those with diabetes mellitus. In the final follow-up survey, recurrence of infection was not reported.
CONCLUSION
A two-stage approach to primary knee arthroplasty with recurrent septic arthritis is a useful method, because it showed good clinical and radiologic results and favorable subjective assessment.
Keyword
MeSH Terms
Figure
-

Figure 1 Intraoperative photograph (debridement of synovium and infected tissue).
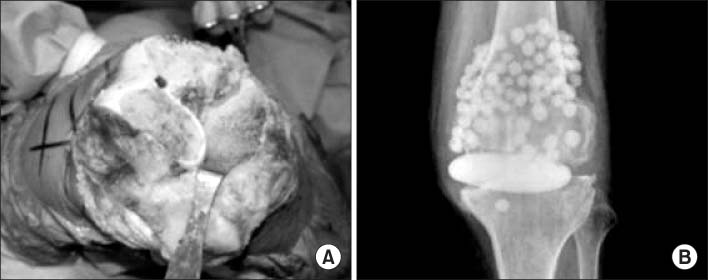
Figure 2 Intraoperative photograph. (A) Bone cutting on distal femur and proximal tibia. (B) Insertion of an antibiotic-impregnated cement spacer block and beads.
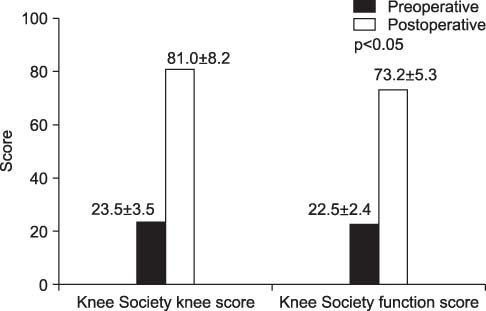
Figure 3 Change of the Knee Society knee score and function score.

Figure 4 Postoperative Knee Society knee score and function score according to the causative organism. MRSA, Methicillin resistant Staphylococcus aureus.
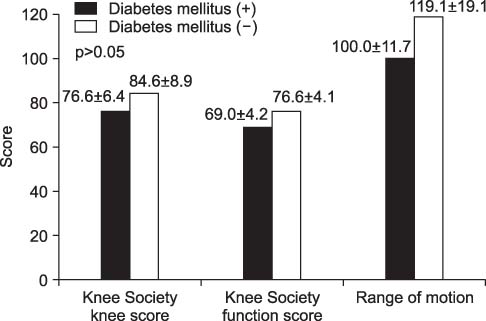
Figure 5 Postoperative clinical outcomes according to the underlying disease (diabetes mellitus).
Reference
-
1. Molloy A, Laing A, O'Shea K, Bell L, O'Rourke K. The complications of septic arthritis in the elderly. Aging Clin Exp Res. 2010; 22:270–273.
Article2. Shemesh S, Heller S, Salai M, Velkes S. Septic arthritis of the knee following intraarticular injections in elderly patients: report of six patients. Isr Med Assoc J. 2011; 13:757–760.3. Vincent GM, Amirault JD. Septic arthritis in the elderly. Clin Orthop Relat Res. 1990; 251:241–245.
Article4. Ivey M, Clark R. Arthroscopic debridement of the knee for septic arthritis. Clin Orthop Relat Res. 1985; 199:201–206.
Article5. Jerosch J, Hoffstetter I, Schröder M, Castro WH. Septic arthritis: arthroscopic management with local antibiotic treatment. Acta Orthop Belg. 1995; 61:126–134.6. Benson ER, Resine ST, Lewis CG. Functional outcome of arthrodesis for failed total knee arthroplasty. Orthopedics. 1998; 21:875–879.
Article7. Knutson K, Lindstrand A, Lidgren L. Arthrodesis for failed knee arthroplasty. A report of 20 cases. J Bone Joint Surg Br. 1985; 67:47–52.
Article8. Thiery JA. Arthroscopic drainage in septic arthritides of the knee: a multicenter study. Arthroscopy. 1989; 5:65–69.
Article9. Katz LM, Lewis RJ, Borenstein DG. Successful joint arthroplasty following Proteus morganii (Morganella morganii) septic arthritis: a four-year study. Arthritis Rheum. 1987; 30:583–585.10. Windsor RE, Insall JN, Urs WK, Miller DV, Brause BD. Two-stage reimplantation for the salvage of total knee arthroplasty complicated by infection. Further follow-up and refinement of indications. J Bone Joint Surg Am. 1990; 72:272–278.
Article11. Insall JN, Thompson FM, Brause BD. Two-stage reimplantation for the salvage of infected total knee arthroplasty. 1983. J Bone Joint Surg Am. 2002; 84:490.12. Anthony A, Mascioli ALP. Infectious arthritis. In : Campbell WC, Canale ST, Beaty JH, editors. Campbell's operative orthopaedics. Philadelphia: Elsevier/Mosby;2013. p. 749–774.13. Broy SB, Schmid FR. A comparison of medical drainage (needle aspiration) and surgical drainage (arthrotomy or arthroscopy) in the initial treatment of infected joints. Clin Rheum Dis. 1986; 12:501–522.
Article14. Goldenberg DL. Septic arthritis. Lancet. 1998; 351:197–202.
Article15. Farrell MJ Jr, Bryan RS. Total knee arthroplasty after septic arthritis. Orthop Clin North Am. 1975; 6:1057–1062.
Article16. Tice AD. Outpatient parenteral antimicrobial therapy for osteomyelitis. Infect Dis Clin North Am. 1998; 12:903–919.
Article17. Pring DJ, Marks L, Angel JC. Mobility after amputation for failed knee replacement. J Bone Joint Surg Br. 1988; 70:770–771.
Article18. Nazarian DG, de Jesus D, McGuigan F, Booth RE Jr. A two-stage approach to primary knee arthroplasty in the infected arthritic knee. J Arthroplasty. 2003; 18:7 Suppl 1. 16–21.
Article19. Kirpalani PA, In Y, Choi NY, Koh HS, Kim JM, Han CW. Two-stage total knee arthroplasty for non-salvageable septic arthritis in diabetes mellitus patients. Acta Orthop Belg. 2005; 71:315–320.20. Bauer T, Lacoste S, Lhotellier L, Mamoudy P, Lortat-Jacob A, Hardy P. Arthroplasty following a septic arthritis history: a 53 cases series. Orthop Traumatol Surg Res. 2010; 96:840–843.
Article21. Mirza AH, Noble J, Teanby D. Infected knee treated by total knee arthroplasty. Knee. 2000; 7:171–174.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Late-Onset Infection of a Total Knee Arthroplasty Caused by Monomicrobial Klebsiella pneumoniae in a Patient with a Periprosthetic Fracture
- Total Knee Arthroplasty in Rheumatoid Arthritis
- Compartment Syndrome of the Thigh Following Manipulation to Treat Knee Stiffness after Total Knee Arthroplasty
- Total Knee Replacement Arthroplasty in Rheumatoid Arthritis and Osteoarthritis
- Total knee replacement arthroplasty in hemophilic arthritis: 2 cases report
