Clinical Effect of Surgical Treatment within 12 Months for Ankylosed Elbow Associated with Heterotopic Ossification
- Affiliations
-
- 1Department of Orthopedic Surgery, Chungbuk National University School of Medicine, Cheongju, Korea. carm0916@hanmail.net
- KMID: 2185161
- DOI: http://doi.org/10.4055/jkoa.2014.49.6.471
Abstract
- Five patients presented with a limited range of motion in their elbow associated with heterotopic ossification. All of these patients underwent surgery within one year. Removal of heterotopic ossification and a posterior capsular release was performed within ten months on average after the initial injury. Each patient postoperatively received prophylaxis consisting of a single-shot radiation of 700 cGY and administration of nonsteroidal anti-inflammatory drugs (NSAIDs) for four weeks on average. With a median follow up period of 21 months, five patients had no radiographic evidence of recurrence. The arc of flexion-extension increased from an average of 64 degrees preoperatively to 133 degrees at the latest follow up. A 12- to 18-month period is generally recommended as necessary for an operation on an ankylosed elbow associated with heterotopic ossification. However, the operative treatment, together with radiation therapy and NSAIDs administration, showed good results within 12 months.
Keyword
MeSH Terms
Figure
-

Figure 1 A 29-year-old male who received conservative treatment for a radial head fracture showed a heterotopic ossification with partial ankylosis around the elbow. (A) Preoperatively, he showed a flexion contracture of approximately 45 degrees and further flexion of approximately 85 degrees in his left elbow. (B) At three months after the injury, x-ray images showed a heterotopic ossification at the posterior and medial side of the elbow. (C) There was no change between x-ray images at month 7 and month 8 (arrows). (D) At 31 months after removal of the heterotopic ossification, follow-up x-ray images showed no evidence for a recurrence of heterotopic ossification. (E) At 31 months postoperatively, the range of motion was approximately 130 degrees compared to 40 degrees preoperatively.
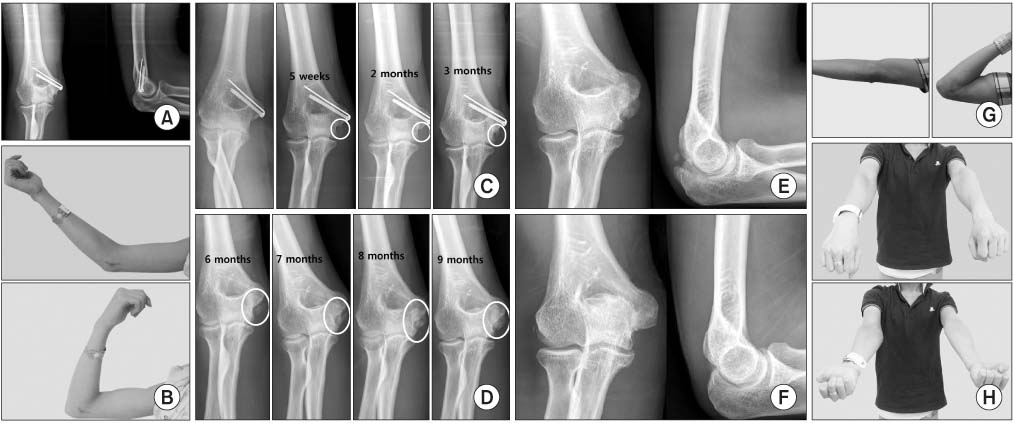
Figure 2 A 24-year-old male with a previous history of open reduction and internal fixation of a medial epicondylar fracture presented with a heterotopic ossification around the elbow. (A) Initially, surgical treatment was administered for the fracture of the medial humeral epicondyle. (B) Preoperatively, the patient showed a flexion contracture of approximately 50 degrees and further flexion of approximately 95 degrees at his left elbow. (C) Five weeks after the initial injury, the heterotopic ossification had emerged on the medial side and the size was gradually increased (circles). (D) Six months after the injury, x-ray images showed a heterotopic ossification at the posterior and medial side of the elbow, which was gradually increased (circles). (E) Ten months after the injury, x-ray images showed matured heterotopic ossification at the posterior and medial side of the elbow. (F) Twelve months after removal of the heterotopic ossification, follow-up x-ray images showed no evidence of recurrence of heterotopic ossification. (G) Twelve months postoperatively, the patient's range of flexion-extension motion was approximately 135 degrees, compared to 45 degrees preoperatively. (H) At 12 months after the operation, he showed an almost normal range of rotation, compared to 100 degrees preoperatively.
Reference
-
1. Garland DE, Hanscom DA, Keenan MA, Smith C, Moore T. Resection of heterotopic ossification in the adult with head trauma. J Bone Joint Surg Am. 1985; 67:1261–1269.
Article2. Hoffer MM, Brody G, Ferlic F. Excision of heterotopic ossification about elbows in patients with thermal injury. J Trauma. 1978; 18:667–670.
Article3. Hastings H 2nd, Graham TJ. The classification and treatment of heterotopic ossification about the elbow and forearm. Hand Clin. 1994; 10:417–437.
Article4. Cauchoix J, Deburge A. Elbow arthrolysis in post-traumatic rigidities. Acta Orthop Belg. 1975; 41:385–392.5. Baek GH, Chung MS, Kim JH, et al. Clinical effects of surgical arthrolysis and radiotherapy for ankylosed elbow with heterotopic ossification. J Korean Soc Surg Hand. 2001; 6:83–89.6. Park MJ, Kim HG, Lee JY. Surgical treatment of post-traumatic elbow stiffness. J Korean Orthop Assoc. 2003; 38:54–59.
Article7. Maender C, Sahajpal D, Wright TW. Treatment of heterotopic ossification of the elbow following burn injury: recommendations for surgical excision and perioperative prophylaxis using radiation therapy. J Shoulder Elbow Surg. 2010; 19:1269–1275.
Article8. Hamid N, Ashraf N, Bosse MJ, et al. Radiation therapy for heterotopic ossification prophylaxis acutely after elbow trauma: a prospective randomized study. J Bone Joint Surg Am. 2010; 92:2032–2038.9. Salazar D, Golz A, Israel H, Marra G. Heterotopic ossification of the elbow treated with surgical resection: risk factors, bony ankylosis, and complications. Clin Orthop Relat Res. 2014; 472:2269–2275.
Article10. Burd TA, Hughes MS, Anglen JO. Heterotopic ossification prophylaxis with indomethacin increases the risk of long-bone nonunion. J Bone Joint Surg Br. 2003; 85:700–705.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Heterotopic Ossification of the Elbow after Medial Epicondylectomy
- Total Ankylosis by Heterotopic Ossification in an Adolescent Anterior Trans-olecranon Fracture Dislocation: A Case Report
- Osteomyelitis in Heterotopic Ossification after Trochanteric Pressure Sore Reconstruction: A Case Report
- Heterotopic Ossification in Post-Burn Scar Contracture of the Wrist
- Heterotopic Ossification of a Partially Ruptured Achilles Tendon (A Case Report)
