Results of Re-Excision Following Unplanned Excision of Soft Tissue Sarcoma: Comparison with the Group of Planned Excision
- Affiliations
-
- 1Department of Orthopedic Surgery, Yeungnam University College of Medicine, Daegu, Korea. shinds@med.yu.ac.kr
- KMID: 2185156
- DOI: http://doi.org/10.4055/jkoa.2014.49.6.431
Abstract
- PURPOSE
This study was designed to investigate the clinical and oncological results of the unplanned excision group, and to compare the results with those of the planned excision group.
MATERIALS AND METHODS
A total of 41 patients who underwent re-excision of sarcoma in Yeungnam University Medical Center, from January 2000 to December 2012, after unplanned excision in local medical centers were reviewed retrospectively. We analyzed the clinical and oncological results according to age, gender, tumor size, depth, and locations. As a control group of planned excision, 81 patients with a similar state, were selected and reviewed among the group of 480 patients who underwent planned excision during the same period. We then compared the results of the two groups.
RESULTS
In the unplanned excision group, only the age factor was statistically significant to survival (p=0.048). In comparison of clinical and oncological results of the unplanned and planned excision groups, recurrence rate was 11.1% in the unplanned group, 10.5% in the planned group and did not show statistical significance (p=0.18). Survival rate was 74% in the unplanned group, 76.6% in the planned group and did not show statistical significance (p=0.06). Necessity of additional surgery for coverage of soft tissue defects was 46% in the unplanned group, 14% in the planned group and showed statistical significance (p=0.00).
CONCLUSION
No significant difference in survival and local recurrence rate was observed between the groups of re-excision with microscopic remnant tumor after unplanned excision and planned excision. However, unplanned excision might lead to unnecessary additional surgery like skin-graft, skin-flap if it were planned.
Keyword
MeSH Terms
Figure
-
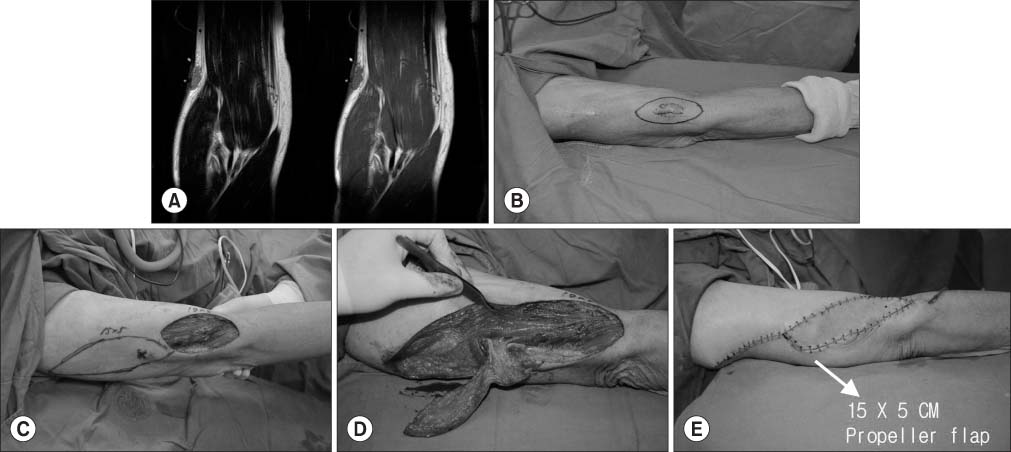
Figure 1 A 76-year-old male who underwent unplanned excision underwent wide re-excision and a residual tumor was confirmed via frozen biopsy. If a residual tumor was not found or the tumor was enough for a wide margin, the excision was closed. (A) Coronal view of the magnetic resonance imaging image taken after an unplanned surgical treatment. (B) Longest diameter of postoperative scar (1.5×2.0 cm). It required a wider excision than the initial scar. (C) Wide excision including the previous scar. (D, E) Propeller flap for wound closure.

Figure 2 (A) Comparison between the planned group and the unplanned group. (B) Overall and event free recurrence rate. Five-year recurrence rate was 11.1% in the unplanned group, 10.5% in the planned group. (C) Overall and event free survival rate. Five-year survival rate was 74% in the unplanned group, 76.6% in the planned group.
Reference
-
1. Kawaguchi N, Ahmed AR, Matsumoto S, Manabe J, Matsushita Y. The concept of curative margin in surgery for bone and soft tissue sarcoma. Clin Orthop Relat Res. 2004; 419:165–172.
Article2. Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin. 2007; 57:43–66.
Article3. Giuliano AE, Eilber FR. The rationale for planned reoperation after unplanned total excision of soft-tissue sarcomas. J Clin Oncol. 1985; 3:1344–1348.
Article4. Davis AM, Kandel RA, Wunder JS, et al. The impact of residual disease on local recurrence in patients treated by initial unplanned resection for soft tissue sarcoma of the extremity. J Surg Oncol. 1997; 66:81–87.
Article5. Noria S, Davis A, Kandel R, et al. Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J Bone Joint Surg Am. 1996; 78:650–655.6. Potter BK, Adams SC, Pitcher JD Jr, Temple HT. Local recurrence of disease after unplanned excisions of high-grade soft tissue sarcomas. Clin Orthop Relat Res. 2008; 466:3093–3100.
Article7. Kawaguchi N, Matumoto S, Manabe J. New method of evaluating the surgical margin and safety margin for musculoskeletal sarcoma, analysed on the basis of 457 surgical cases. J Cancer Res Clin Oncol. 1995; 121:555–563.
Article8. Chandrasekar CR, Wafa H, Grimer RJ, Carter SR, Tillman RM, Abudu A. The effect of an unplanned excision of a soft-tissue sarcoma on prognosis. J Bone Joint Surg Br. 2008; 90:203–208.
Article9. Manoso MW, Frassica DA, Deune EG, Frassica FJ. Outcomes of re-excision after unplanned excisions of soft-tissue sarcomas. J Surg Oncol. 2005; 91:153–158.
Article10. Cho WH, Song WS, Park JH, et al. The result of re-excision following unplanned excision of soft tissue sarcoma of the extremities. J Korean Orthop Assoc. 2005; 40:490–495.
Article11. Jeon DG, Lee JS, Kim SJ, Gwak BJ, Cho WH, Lee SY. Stage oriented analysis of soft tissue sarcomas. J Korean Orthop Assoc. 1999; 34:673–679.
Article12. Kamada T, Tsujii H, Tsuji H, et al. Working Group for the Bone and Soft Tissue Sarcomas. Efficacy and safety of carbon ion radiotherapy in bone and soft tissue sarcomas. J Clin Oncol. 2002; 20:4466–4471.
Article13. Lewis JJ, Leung D, Espat J, Woodruff JM, Brennan MF. Effect of reresection in extremity soft tissue sarcoma. Ann Surg. 2000; 231:655–663.
Article14. Mankin HJ, Mankin CJ, Simon MA. The hazards of the biopsy, revisited. Members of the Musculoskeletal Tumor Society. J Bone Joint Surg Am. 1996; 78:656–663.15. Pervaiz N, Colterjohn N, Farrokhyar F, Tozer R, Figueredo A, Ghert M. A systematic meta-analysis of randomized controlled trials of adjuvant chemotherapy for localized resectable soft-tissue sarcoma. Cancer. 2008; 113:573–581.
Article16. Clasby R, Tilling K, Smith MA, Fletcher CD. Variable management of soft tissue sarcoma: regional audit with implications for specialist care. Br J Surg. 1997; 84:1692–1696.
Article17. Sugiura H, Takahashi M, Katagiri H, et al. Additional wide resection of malignant soft tissue tumors. Clin Orthop Relat Res. 2002; 394:201–210.
Article18. Qureshi YA, Huddy JR, Miller JD, Strauss DC, Thomas JM, Hayes AJ. Unplanned excision of soft tissue sarcoma results in increased rates of local recurrence despite full further oncological treatment. Ann Surg Oncol. 2012; 19:871–877.
Article19. Fiore M, Casali PG, Miceli R, et al. Prognostic effect of re-excision in adult soft tissue sarcoma of the extremity. Ann Surg Oncol. 2006; 13:110–117.
Article20. Goodlad JR, Fletcher CD, Smith MA. Surgical resection of primary soft-tissue sarcoma. Incidence of residual tumour in 95 patients needing re-excision after local resection. J Bone Joint Surg Br. 1996; 78:658–661.21. Pisters PW, Harrison LB, Leung DH, Woodruff JM, Casper ES, Brennan MF. Long-term results of a prospective randomized trial of adjuvant brachytherapy in soft tissue sarcoma. J Clin Oncol. 1996; 14:859–868.
Article22. Brennan MF, Casper ES, Harrison LB, Shiu MH, Gaynor J, Hajdu SI. The role of multimodality therapy in soft-tissue sarcoma. Ann Surg. 1991; 214:328–336. discussion 336-8.
Article23. Collin C, Hajdu S, Godbold J, Friedrich C, Brennan MF. Localized operable soft tissue sarcoma of the upper extremity. Presentation, management, and factors affecting local recurrence in 108 patients. Ann Surg. 1987; 205:331–339.24. Nishimura A, Matsumine A, Asanuma K, et al. The adverse effect of an unplanned surgical excision of foot soft tissue sarcoma. World J Surg Oncol. 2011; 9:160.
Article25. Hoshi M, Ieguchi M, Takami M, et al. Clinical problems after initial unplanned resection of sarcoma. Jpn J Clin Oncol. 2008; 38:701–709.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Unplanned Excision of Soft Tissue Sarcoma: Patient Profile and Treatment Outcomes
- The Result of Re-excision Following Unplanned Excision of Soft Tissue Sarcoma of the Extremities
- Distinct Clinical Characteristics of Unplanned Excision in Synovial Sarcoma
- Diagnostic Accuracy of Imaging Study and the Impact of Clinical Risk Factors on the Presence of Residual Tumor Following Unplanned Excision of Soft Tissue Sarcomas
- Reconstruction of Defect After Wide Excision of Malignant Soft Tissue Tumor of Limb Using Free Flap
