J Korean Med Assoc.
2006 Jan;49(1):53-60. 10.5124/jkma.2006.49.1.53.
Nocturnal Enuresis
- Affiliations
-
- 1Department of Urology, Chung-Ang University College of Medicine and Hospital, Korea. kim14141@hananet.net
- KMID: 2184636
- DOI: http://doi.org/10.5124/jkma.2006.49.1.53
Abstract
- Nocturnal enuresis is the second most common chronic health problem in children following allergy. The prevalence of nocturnal enuresis in different age groups is about the same in all parts of the world. It can be stated that nocturnal enuresis is a clinical problem for the child and the family as well when the child is wetting the bed at least one night every month. With this definition, about 10% of 7-year-old children have nocturnal enuresis. Historically, a remarkable progress has been made in the mid-eighties. Previously, bedwetting was looked upon as a trivial condition, hardly worthy of serious medical assessment and management. In 1985, however, a study from Aarhus in Denmark drew a strong attention to bedwetting in the medical community worldwide by suggesting that nocturnal enuresis may be caused by nocturnal polyuria, which in turn depends on an insufficient production of antidiuretic hormone (vasopressin) during the sleeping hours. Since then, nocturnal enuresis has turned out to be an unexpectedly fruitful area for research, producing hundreds of scientific reports. Regarding its pathophysiology, it is becoming clear that two thirds of children with nocturnal enuresis have nocturnal polyuria due to an inadequate vasopressin secretion during sleep. In addition, ongoing studies suggest that there may be bladder problems (unstable bladder) or arousal disorder underlying nocturnal enuresis. Nocturnal enuresis should be taken seriously by physicians and needs intervention when the child expresses a desire to sleep dry, usually around 5 years of age.
MeSH Terms
Figure
-
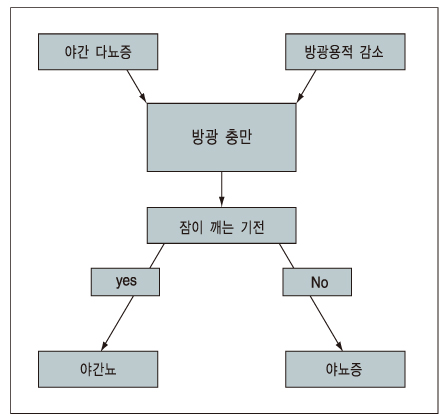
Figure 1 Pathogenesis of nocturnal enuresis
Reference
-
1. Nørgaard JP, Pedersen EB, Djurhuus JC. Diurnal anti-diuretic-hormone levels in enuretics. J Urol. 1985. 134:1029–1031.
Article2. Hjalmas K. Nocturnal enuresis: Basic facts and new horizons. Eur Urol. 1998. 33:Suppl 3. 53–57.
Article3. Butler RJ. Annotation: night wetting in children: psychological aspects. J Child Psychol Psychiat. 1998. 39:453–463.
Article4. Nørgaard JP, van Gool JD, Hjälmås K, Djurhuus JC, Hellström AL. Standardization and definitions in lower urinary tract dysfunction in children. Br J Urol. 1998. 81:Suppl 3. 1–16.
Article5. Chiozza ML, Bernardinelli L, Caione P, Del Gade R, Ferrara P, Giorgi PL, et al. An Italian epidemiological multicentre study of nocturnal enuresis. Br J Urol. 1998. 81:Suppl. 86–90.
Article7. Kim KD. The Korean Enuresis Association. An epidemiological study of nocturnal enuresis in Korean adults. 2005. In : APAPU meeting; Abstract No. 27: 62.8. Hjalmas K, Arnold T, Bower W, Caione I, Chiozza M, Yeung CK, et al. Nocturnal enuresis: An international evidence based management strategy. J Urol. 2004. 171:2545–2561.
Article13. Mowrer OH, Mowrer WM. Enuresis: A method for its study and treatment. Amer. J Orthopsych. 1938. 8:436–440.14. Oredsson AF, Jorgensen TM. Changes in nocturnal bladder capacity during treatment with the bell and pad for monosymptomatic nocturnal enuresis. J Urol. 1998. 160:166–172.
Article16. Radmayr C, Schlager B, Studen M, Bartsch G. Prospective randomized trial using laser acupuncture versus desmopressin in the treatment of nocturnal enuresis. Eur Urol. 2001. 40:201–205.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Oxybutynin Hydrochloride in 3 Cases of Clozapine Induced Nocturnal Enuresis
- The Relations between Enuresis in Childhood and Nocturnal Polyuria Syndrome in Adult Life
- Management of patients with refractory nocturnal enuresis
- Pharmacological therapy of nocturnal enuresis
- Circadian Rhythm of ADH, Hypercalciuria, and Solute Diuresis as Pathogenesis of Enuresis
