Periprosthetic Fracture after Hook Plate Fixation in Neer Type II Distal Clavicle Fracture: A Report of 3 Cases
- Affiliations
-
- 1Department of Anatomy, Chung-Ang University College of Medicine, Seoul, Korea.
- 2Department of Orthopaedic Surgery, Myongji Hospital, Seonam University School of Medicine, Goyang, Korea. doctoryub@naver.com
- KMID: 2183766
- DOI: http://doi.org/10.12671/jkfs.2016.29.1.55
Abstract
- Hook plate fixation is a treatment method for the displaced distal clavicle fracture with favorable results regarding bone union and shoulder function, however possible complications include impingement syndromes, subacrormial erosions, acromial fractures, and periprosthetic fractures. In this report, we observed 3 cases of periprosthetic fracture after hook plate fixation. All cases of periprosthetic fractures were initiated at the medial end screw holes. The causes of these periprosthetic fractures appeared to be the off centered fixation of medial end screws near the anterior or posterior cortex which were specific during operations with hook plates with more than 6 holes and the increased stress on the medial end screw by over-reduced or inferiorly reduced position of the distal end of the clavicle by the hook plate.
Keyword
MeSH Terms
Figure
-

Fig. 1 (A) Neer type IIa distal clavicle fracture. (B) Open reduction and internal fixation with clavicular hook plate. (C) Medial end of the clavicular hook plate had migrated superiorly and medial end screw lost the fixation to inferior cortex (white arrow). (D) Axial cut of 2-dimensional computed tomography. The medial end fracture at the medial screw of the hook plate was observed (white arrow). (E) Open reduction and internal fixation with clavicular anatomical plate for newly onset fracture after removal of the hook plate.
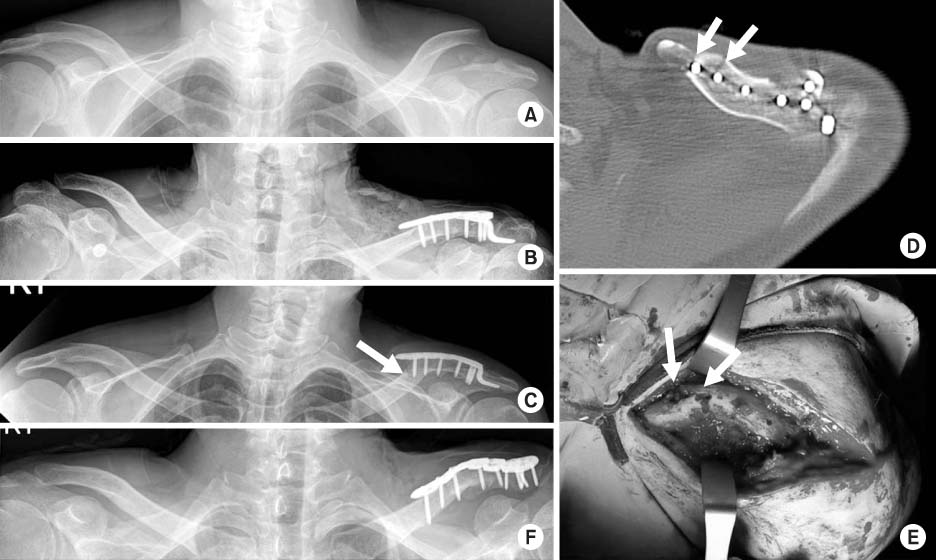
Fig. 2 (A) Neer type IIa distal clavicle fracture. (B) Open reduction and internal fixation with clavicular hook plate. (C) Fracture at the medial screw of the hook plate was observed and medial end screw lost the fixation to inferior cortex (white arrow). (D) Axial cut of 2-dimensional computed tomography (CT) showed the fracture line communicating the medial two holes of the hook plate (2 white arrows). (E) Clinical photo corresponded to the CT findings (2 white arrows). (F) Open reduction and internal fixation with clavicular plate with cerclage wiring with No. 2 fiber wire between coracoid process and clavicular shaft.

Fig. 3 (A) Neer type IIb distal clavicle fracture. (B) Open reduction and internal fixation with clavicular hook plate. (C) Medial end of the plate had migrated superiorly (white arrow). (D) Axial cut of 2-dimensional computed tomography of the medial end fracture. The fracture started from inferior portion of medial end screw to the unused drill hole which was located anterolaterally to the medial end screw (2 white arrows). (E) Open reduction and internal fixation with clavicular anatomical plate and reconstruction plate as well as K-wires was performed for the revision surgery.
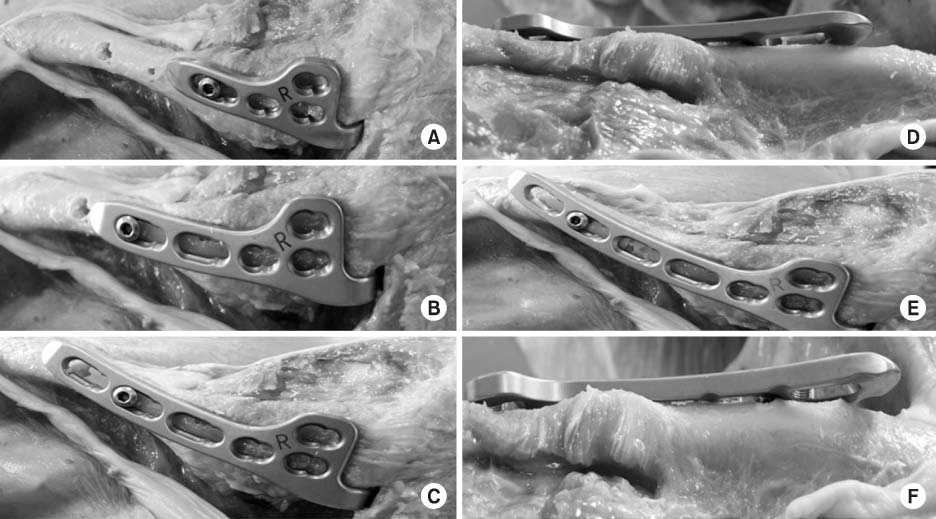
Fig. 4 (A) A 4-hole clavicular hook plate was applied and all holes were in appropriate position on the clavicle. (B) A 5-hole clavicular hook plate was applied and all holes were in appropriate position on the clavicle. (C, D) A 6-hole clavicular hook plate was applied and the most medial hole was slightly off centered and anteriorly positioned to the clavicle (C: from cranial to caudal view, D: from caudal to cranial view). (E, F) A 7-hole clavicular hook plate was applied and the most medial hole was definitely off centered and anteriorly positioned to the clavicle (E: from cranial to caudal view, F: from caudal to cranial view).
Cited by 1 articles
-
Comparison of Locking Compression Plate Superior Anterior Clavicle Plate with Suture Augmentation and Hook Plate for Treatment of Distal Clavicle Fractures
Jun-Cheol Choi, Woo-Suk Song, Woo-Sung Kim, Jeong-Muk Kim, Chan-Woong Byun
Arch Hand Microsurg. 2017;22(4):247-255. doi: 10.12790/ahm.2017.22.4.247.
Reference
-
1. Neer CS 2nd. Fracture of the distal clavicle with detachment of the coracoclavicular ligaments in adults. J Trauma. 1963; 3:99–110.
Article2. Oh JH, Kim SH, Lee JH, Shin SH, Gong HS. Treatment of distal clavicle fracture: a systematic review of treatment modalities in 425 fractures. Arch Orthop Trauma Surg. 2011; 131:525–533.
Article3. Tambe AD, Motkur P, Qamar A, Drew S, Turner SM. Fractures of the distal third of the clavicle treated by hook plating. Int Orthop. 2006; 30:7–10.
Article4. Fann CY, Chiu FY, Chuang TY, Chen CM, Chen TH. Transacromial Knowles pin in the treatment of Neer type 2 distal clavicle fractures. A prospective evaluation of 32 cases. J Trauma. 2004; 56:1102–1105.5. Good DW, Lui DF, Leonard M, Morris S, McElwain JP. Clavicle hook plate fixation for displaced lateral-third clavicle fractures (Neer type II): a functional outcome study. J Shoulder Elbow Surg. 2012; 21:1045–1048.
Article6. Meda PV, Machani B, Sinopidis C, Braithwaite I, Brownson P, Frostick SP. Clavicular hook plate for lateral end fractures:- a prospective study. Injury. 2006; 37:277–283.
Article7. Flinkkilä T, Ristiniemi J, Hyvönen P, Hämäläinen M. Surgical treatment of unstable fractures of the distal clavicle: a comparative study of Kirschner wire and clavicular hook plate fixation. Acta Orthop Scand. 2002; 73:50–53.
Article8. Nadarajah R, Mahaluxmivala J, Amin A, Goodier DW. Clavicular hook-plate: complications of retaining the implant. Injury. 2005; 36:681–683.
Article9. Charity RM, Haidar SG, Ghosh S, Tillu AB. Fixation failure of the clavicular hook plate: a report of three cases. J Orthop Surg (Hong Kong). 2006; 14:333–335.
Article10. Ding M, Ni J, Hu J, Song D. Rare complication of clavicular hook plate: clavicle fracture at the medial end of the plate. J Shoulder Elbow Surg. 2011; 20:e18–e20.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Periprosthetic Clavicle Shaft Fracture After Treatment of Type V Distal Clavicle Fracture Using a Hook Plate: A Report of Two Cases
- Mini-T Plate Fixation for Neer Type II Distal Clavicle Fracture
- Surgical Treatment of Unstable Distal Clavicle Fractures: Comparison of Transacromial Pin Fixation and Hook Plate Fixation
- Comparison of Results of Tension Band Wire and Hook Plate in the Treatment of Unstable Fractures of the Distal Clavicle
- Complications of Hook-Plate Fixation for Distal Clavicle Fractures
