J Gastric Cancer.
2014 Dec;14(4):229-237. 10.5230/jgc.2014.14.4.229.
Uncut Roux-en-Y Reconstruction after Laparoscopic Distal Gastrectomy Can Be a Favorable Method in Terms of Gastritis, Bile Reflux, and Gastric Residue
- Affiliations
-
- 1Department of Surgery, Soonchunhyang University Hospital Seoul, Seoul, Korea. yjgs1997@gmail.com
- KMID: 2183646
- DOI: http://doi.org/10.5230/jgc.2014.14.4.229
Abstract
- PURPOSE
Laparoscopic distal gastrectomy (LDG) is a well-established procedure for the treatment of early gastric cancer. Several reconstruction methods can be adopted after LDG according to tumor characteristics and surgeon preference. This study aimed to compare the remnant gastric functions after different reconstructions.
MATERIALS AND METHODS
In total, 221 patients who underwent LDG between March 2005 and October 2013 were reviewed retrospectively. The patients were classified into four groups based on the reconstructive procedure: Billroth I (BI) anastomosis, Billroth II (BII) with Braun anastomosis, Roux-en-Y (RY) reconstruction, or uncut RY reconstruction. Patient demographics, surgical outcomes, and postoperative endoscopic findings were reviewed and compared among groups.
RESULTS
Endoscopic evaluations at 11.8+/-3.8 months postoperatively showed less frequent gastritis and bile reflux in the remnant stomach in the RY group compared to the BI and BII groups. There was no significant difference in the gastric residue among the BI, BII, and RY groups. The incidence of gastritis and bile reflux in the uncut RY group was similar to that in the RY group, while residual gastric content in the uncut RY group was significantly smaller and less frequently observed than that in the RY group (5.8% versus 35.3%, P=0.010).
CONCLUSIONS
RY and uncut RY reconstructions are equally superior to BI and BII with Braun anastomoses in terms of gastritis and bile reflux in the remnant stomach. Furthermore, uncut RY reconstruction showed improved stasis compared to conventional RY gastrojejunostomy. Uncut RY reconstruction can be a favorable reconstructive procedure after LDG.
Keyword
MeSH Terms
Figure
-
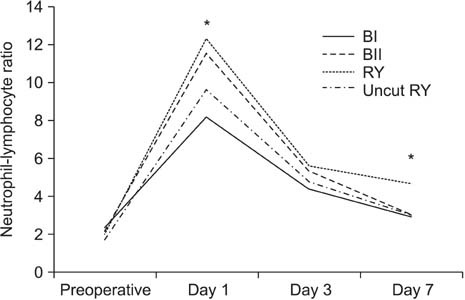
Fig. 1 Systemic inflammatory response after surgery according to the reconstructive procedures. BI = Billroth I gastroduodenostomy; BII = Billroth II gastrojejunostomy; RY = Roux-en-Y reconstruction. *P<0.05; by one-way analysis of variance.
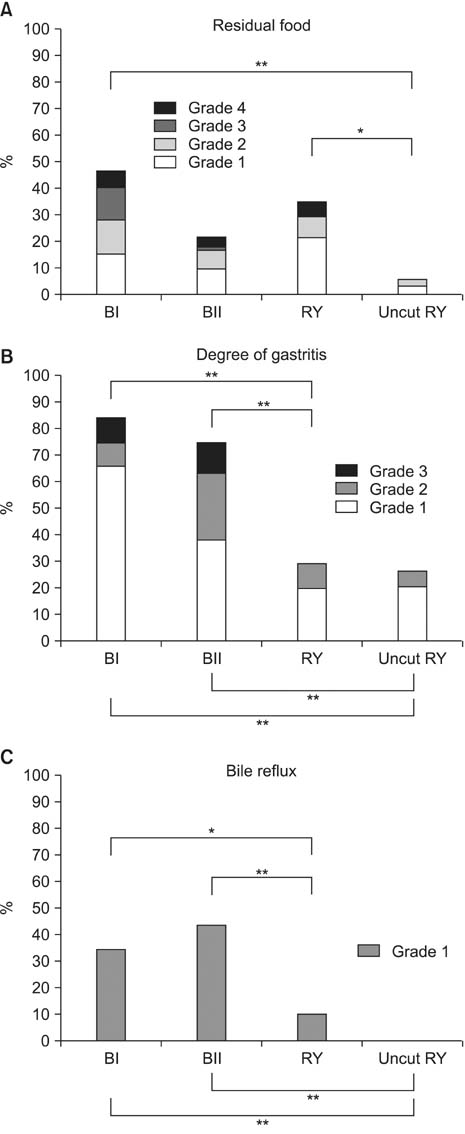
Fig. 2 Comparison of endoscopic findings after different reconstruction methods following laparoscopic distal gastrectomy: residual food (A), degree of gastritis (B), and bile reflux (C). BI = Billroth I gastroduodenostomy; BII = Billroth II gastrojejunostomy; RY = Roux-en-Y reconstruction. *P<0.05; **P<0.005 by Pearson's chi-square test or Fisher's exact test.
Reference
-
1. Jung KW, Won YJ, Kong HJ, Oh CM, Lee DH, Lee JS. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2011. Cancer Res Treat. 2014; 46:109–123.
Article2. Kim YG, Kong SH, Oh SY, Lee KG, Suh YS, Yang JY, et al. Effects of screening on gastric cancer management: comparative analysis of the results in 2006 and in 2011. J Gastric Cancer. 2014; 14:129–134.
Article3. Jeong O, Park YK. Clinicopathological features and surgical treatment of gastric cancer in South Korea: the results of 2009 nationwide survey on surgically treated gastric cancer patients. J Gastric Cancer. 2011; 11:69–77.
Article4. Kim YW, Yoon HM, Yun YH, Nam BH, Eom BW, Baik YH, et al. Long-term outcomes of laparoscopy-assisted distal gastrectomy for early gastric cancer: result of a randomized controlled trial (COACT 0301). Surg Endosc. 2013; 27:4267–4276.
Article5. Kim YW, Baik YH, Yun YH, Nam BH, Kim DH, Choi IJ, et al. Improved quality of life outcomes after laparoscopy-assisted distal gastrectomy for early gastric cancer: results of a prospective randomized clinical trial. Ann Surg. 2008; 248:721–727.
Article6. Yasunaga H, Horiguchi H, Kuwabara K, Matsuda S, Fushimi K, Hashimoto H, et al. Outcomes after laparoscopic or open distal gastrectomy for early-stage gastric cancer: a propensitymatched analysis. Ann Surg. 2013; 257:640–646.
Article7. Washington K. 7th edition of the AJCC cancer staging manual: stomach. Ann Surg Oncol. 2010; 17:3077–3079.
Article8. Han G, Park JY, Kim YJ. Comparison of short-term postoperative outcomes in totally laparoscopic distal gastrectomy versus laparoscopy-assisted distal gastrectomy. J Gastric Cancer. 2014; 14:105–110.
Article9. Yun SC, Choi HJ, Park JY, Kim YJ. Total laparoscopic uncut Roux-en-Y gastrojejunostomy after distal gastrectomy. Am Surg. 2014; 80:E51–E53.
Article10. Wolters U, Wolf T, Stützer H, Schröder T. ASA classification and perioperative variables as predictors of postoperative outcome. Br J Anaesth. 1996; 77:217–222.
Article11. Strasberg SM, Linehan DC, Hawkins WG. The accordion severity grading system of surgical complications. Ann Surg. 2009; 250:177–186.
Article12. Kubo M, Sasako M, Gotoda T, Ono H, Fujishiro M, Saito D, et al. Endoscopic evaluation of the remnant stomach after gastrectomy: proposal for a new classification. Gastric Cancer. 2002; 5:83–89.
Article13. Piessen G, Triboulet JP, Mariette C. Reconstruction after gastrectomy: which technique is best. J Visc Surg. 2010; 147:e273–e283.
Article14. Kumagai K, Shimizu K, Yokoyama N, Aida S, Arima S, Aikou T;. Questionnaire survey regarding the current status and controversial issues concerning reconstruction after gastrectomy in Japan. Surg Today. 2012; 42:411–418.
Article15. Tu BN, Kelly KA. Elimination of the Roux stasis syndrome using a new type of "uncut Roux" limb. Am J Surg. 1995; 170:381–386.
Article16. Morrison P, Miedema BW, Kohler L, Kelly KA. Electrical dysrhythmias in the Roux jejunal limb: cause and treatment. Am J Surg. 1990; 160:252–256.
Article17. Miedema BW, Kelly KA. The Roux stasis syndrome. Treatment by pacing and prevention by use of an 'uncut Roux' limb. Arch Surg. 1992; 127:295–300.18. Tu BN, Sarr MG, Kelly KA. Early clinical results with the uncut Roux reconstruction after gastrectomy: limitations of the stapling technique. Am J Surg. 1995; 170:262–264.
Article19. Cook EJ, Walsh SR, Farooq N, Alberts JC, Justin TA, Keeling NJ. Post-operative neutrophil-lymphocyte ratio predicts complications following colorectal surgery. Int J Surg. 2007; 5:27–30.
Article20. Tabuchi T, Shimazaki J, Satani T, Nakachi T, Watanabe Y, Tabuchi T. The perioperative granulocyte/lymphocyte ratio is a clinically relevant marker of surgical stress in patients with colorectal cancer. Cytokine. 2011; 53:243–248.
Article21. Sharaiha RZ, Halazun KJ, Mirza F, Port JL, Lee PC, Neugut AI, et al. Elevated preoperative neutrophil:lymphocyte ratio as a predictor of postoperative disease recurrence in esophageal cancer. Ann Surg Oncol. 2011; 18:3362–3369.
Article22. Ishizuka M, Nagata H, Takagi K, Iwasaki Y, Kubota K. Combination of platelet count and neutrophil to lymphocyte ratio is a useful predictor of postoperative survival in patients with colorectal cancer. Br J Cancer. 2013; 109:401–407.
Article23. Yamanaka T, Matsumoto S, Teramukai S, Ishiwata R, Nagai Y, Fukushima M. The baseline ratio of neutrophils to lymphocytes is associated with patient prognosis in advanced gastric cancer. Oncology. 2007; 73:215–220.
Article24. Shimada H, Takiguchi N, Kainuma O, Soda H, Ikeda A, Cho A, et al. High preoperative neutrophil-lymphocyte ratio predicts poor survival in patients with gastric cancer. Gastric Cancer. 2010; 13:170–176.
Article25. Ishikawa M, Kitayama J, Kaizaki S, Nakayama H, Ishigami H, Fujii S, et al. Prospective randomized trial comparing Billroth I and Roux-en-Y procedures after distal gastrectomy for gastric carcinoma. World J Surg. 2005; 29:1415–1420.
Article26. Kojima K, Yamada H, Inokuchi M, Kawano T, Sugihara K. A comparison of Roux-en-Y and Billroth-I reconstruction after laparoscopy-assisted distal gastrectomy. Ann Surg. 2008; 247:962–967.
Article27. Inokuchi M, Kojima K, Yamada H, Kato K, Hayashi M, Motoyama K, et al. Long-term outcomes of Roux-en-Y and Billroth-I reconstruction after laparoscopic distal gastrectomy. Gastric Cancer. 2013; 16:67–73.
Article28. Dixon MF, Neville PM, Mapstone NP, Moayyedi P, Axon AT. Bile reflux gastritis and Barrett's oesophagus: further evidence of a role for duodenogastro-oesophageal reflux? Gut. 2001; 49:359–363.
Article29. Theisen J, Peters JH, Fein M, Hughes M, Hagen JA, Demeester SR, et al. The mutagenic potential of duodenoesophageal reflux. Ann Surg. 2005; 241:63–68.
Article30. Mason RC. Duodenogastric reflux in rat gastric carcinoma. Br J Surg. 1986; 73:801–803.
Article31. Kondo K. Duodenogastric reflux and gastric stump carcinoma. Gastric Cancer. 2002; 5:16–22.
Article32. Takiguchi S, Yamamoto K, Hirao M, Imamura H, Fujita J, Yano M, et al. A comparison of postoperative quality of life and dysfunction after Billroth I and Roux-en-Y reconstruction following distal gastrectomy for gastric cancer: results from a multi-institutional RCT. Osaka University Clinical Research Group for Gastroenterological Study. Gastric Cancer. 2012; 15:198–205.
Article33. Vogel SB, Drane WE, Woodward ER. Clinical and radionuclide evaluation of bile diversion by Braun enteroenterostomy: prevention and treatment of alkaline reflux gastritis. An alternative to Roux-en-Y diversion. Ann Surg. 1994; 219:458–465.34. Chan DC, Fan YM, Lin CK, Chen CJ, Chen CY, Chao YC. Roux-en-Y reconstruction after distal gastrectomy to reduce enterogastric reflux and Helicobacter pylori infection. J Gastrointest Surg. 2007; 11:1732–1740.
Article35. Lee MS, Ahn SH, Lee JH, Park do J, Lee HJ, Kim HH, et al. What is the best reconstruction method after distal gastrectomy for gastric cancer. Surg Endosc. 2012; 26:1539–1547.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of an Uncut Roux-en-Y Gastrojejunostomy with a Billroth I Gastroduodenostomy after Totally Laproscopic Distal Gastrectomy
- A Clinical Study of the Uncut Roux-en-Y Gastrojejunostomy Using a Short Roux Limb after Subtotal Gastrectomy
- A Comparison of Outcomes of Three Reconstruction Methods after Laparoscopic Distal Gastrectomy
- Laparoscopic Hiatal Hernia Repair and Roux-en-Y Conversion for Refractory Duodenogastroesophageal Reflux after Billroth I Distal Gastrectomy
- A Novel Roux-en-Y Reconstruction Involving the Use of Two Circular Staplers after Distal Subtotal Gastrectomy for Gastric Cancer
