Full mouth rehabilitation on the patient with class II jaw relation and posterior bite collapse using reestablishment of occlusal vertical dimension: a case report
- Affiliations
-
- 1Department of Prosthodontics, College of Dentistry, Wonkwang University, Iksan, Republic of Korea. stop-it@hanmail.net
- KMID: 2180029
- DOI: http://doi.org/10.14368/jdras.2015.31.3.262
Abstract
- Loss of molar support and abnormal jaw relationship lead to occlusal disharmony and cause pathologic signs. Full mouth rehabilitations with reestablishment of occlusal schemes are needed. In this case, the 75 year-old female patient showed posterior bite collapse, irregular occlusal plane and Class II jaw relationship. By observing her profile and interocclusal distance, she was diagnosed as loss of occlusal vertical dimension. Treatment plan is to restore maxillay class I removable partial denture and mandibular fixed prosthesis and to establish vertical dimension and harmonious occlusal plane. Occlusal vertical dimension of 19 mm, which is obtained by 7.5 mm increase between maxillary right lateral incisor and mandibular canine, was established using temporary prosthesis via diagnostic wax-up. Patient adaptation with newly formed vertical dimension was verified during 8 week follow-up period. Within the information of interim prostheses, final restoration was constructed and delivered. The patient showed sound occlusal scheme and esthetic profile.
Keyword
MeSH Terms
Figure
-

Fig. 1 Panoramic radiograph before treatment.

Fig. 2 Intraoral view after extraction of hopeless teeth. (A) Maxillary occlusal view, (B) Right lateral view, (C) Frontal view, (D) Left lateral view, (E) Mandibular occlusal view.
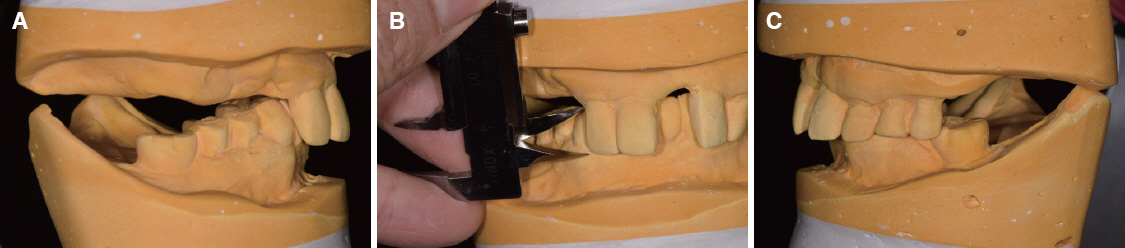
Fig. 3 Mounted diagnostic model analysis. (A) Posterior collapsed bite on right side and mandibular canine had a contact with soft tissue of maxillary palate, (B) Intergingival distance between zenith lines of right maxillary lateral incisor and mandibular canine was 11.5 mm, (C) MICP contact between the maxillary left 2nd bicuspid and mandibular 1st molar.
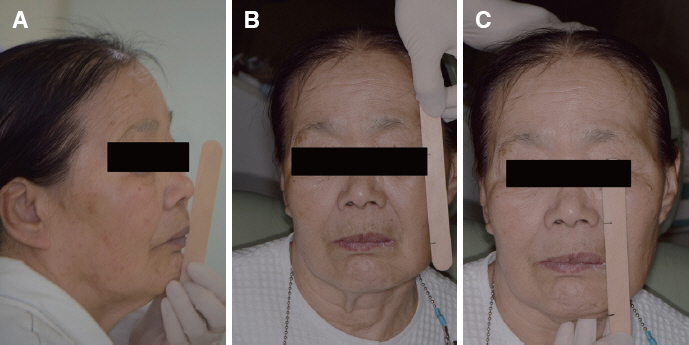
Fig. 4 Determination of vertical dimension. (A) Physiologic resting position, (B) Measurement of distance between the pupil and mouth corner using Willis method, (C) Measurement of length of lower 1/3 of the face using Willis method.
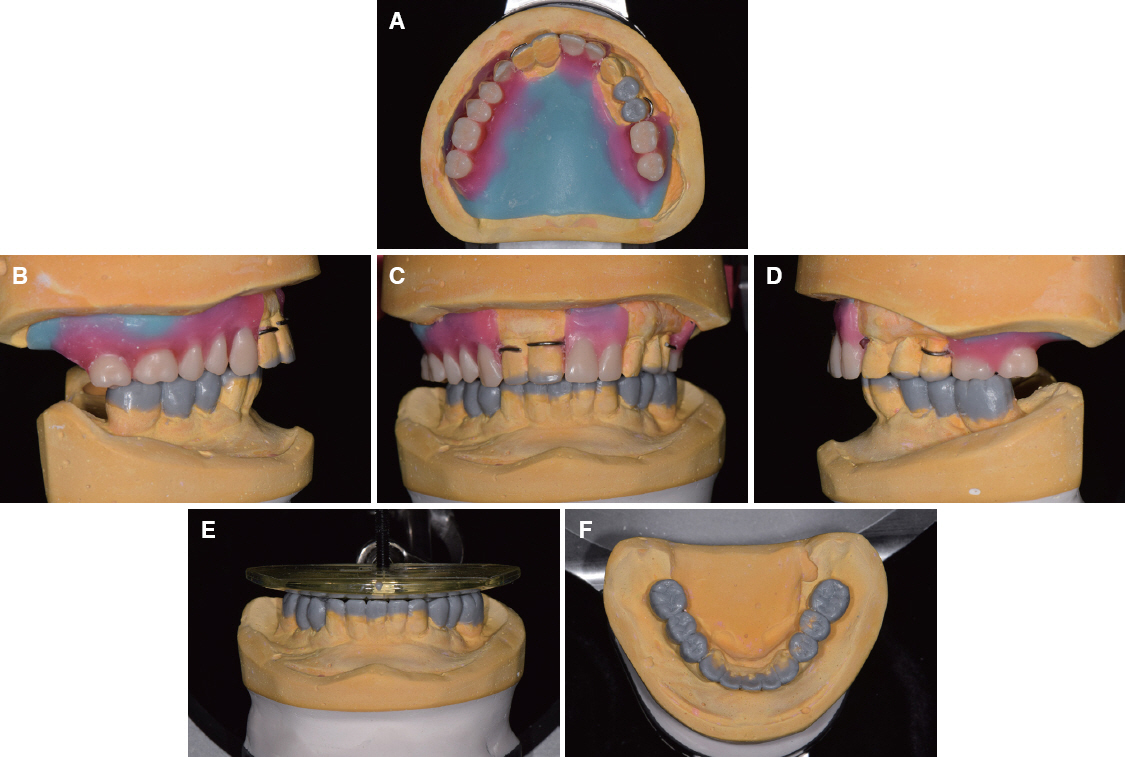
Fig. 5 Diagnostic wax up using new vertical dimension for interim prostheses. (A) Maxillary occlusal view, (B) Right lateral view, (C) Frontal view, (D) Left lateral view, (E) Harmonious occlusal plane establishment using occlusal plane guide, (F) Mandibular occlusal view.
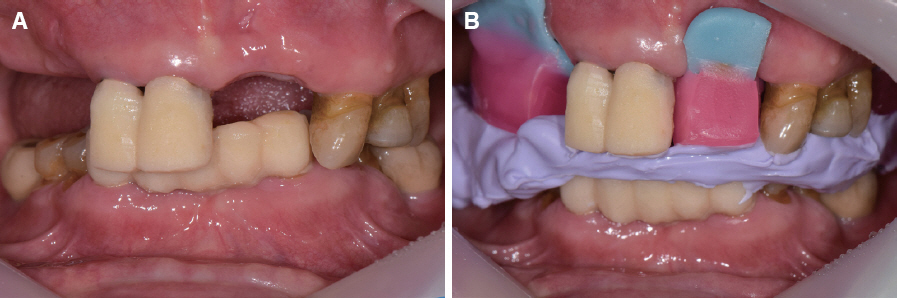
Fig. 6 (A) Newly placed temporary fixed partial denture (FPD) after removal of old FPD, (B) New centric relation record with increased vertical dimension.
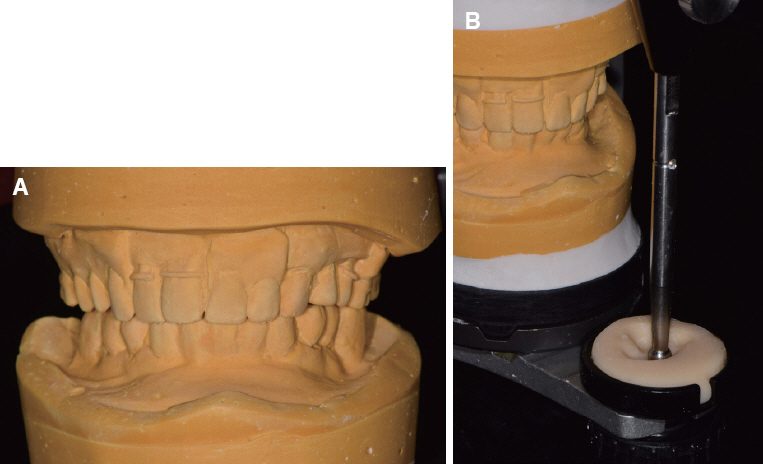
Fig. 7 (A) Mounted models after temporization, (B) Fabrication of customized anterior guide table.

Fig. 8 Abutment preparation for definitive prosthesis. (A) Maxillary occlusal view, (B) Mandibular occlusal view.

Fig. 9 Deivery of definitive FPDs with increased vertical dimension. (A) Maxillary occlusal view, (B) Mandibular occlusal view.
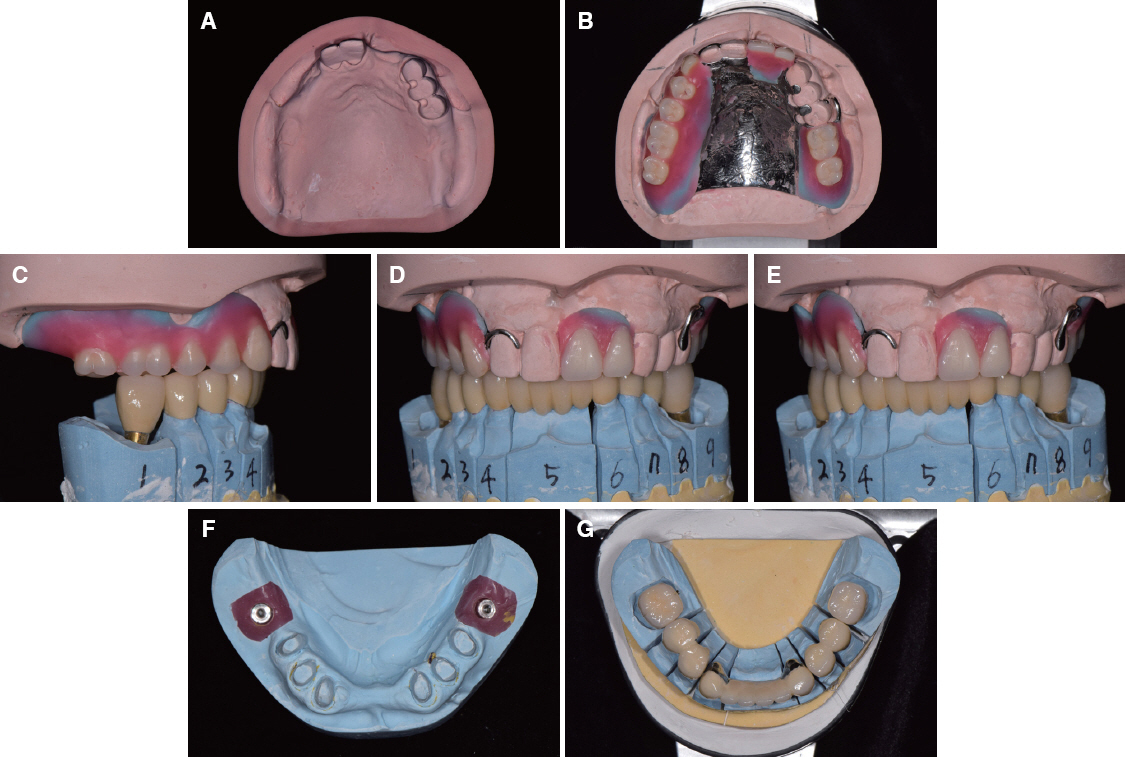
Fig. 10 Definitive prostheses. (A) Maxillary master cast, (B) Maxillary occlusal view of removable partial denture, (C) Right lateral view, (D) Frontal view, (E) Right lateral view, (F) Mandibular working cast, (G) Mandibular occlusal view of metal ceramic restoration.

Fig. 11 Establishment of occlusal scheme. (A) Left lateral movement, (B) Right lateral movement, (C) Protrusion.
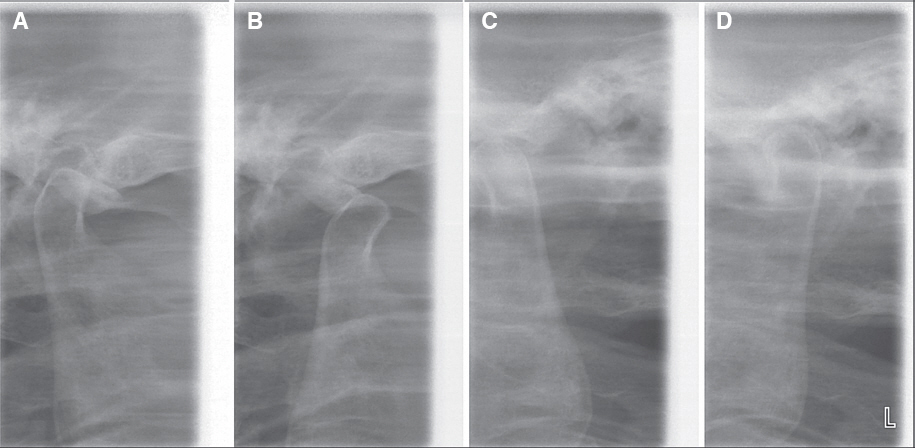
Fig. 12 TMJ radiograph series after treatment. (A) Centric occlusion (Rt side), (B) Maximum opening (Rt side), (C) Maximum opening (Lt side), (D) Centric occlusion (Lt side).
Reference
-
References
1. Verrett RG. Analyzing the etiology of an extremely worn dentition. J Prosthodont. 2001; 10:224–33. DOI: 10.1111/j.1532-849X.2001.00224.x. PMID: 11781971.2. Winstanley RB. A retrospective analysis of the treatment of occlusal disharmony by selective grinding. J Oral Rehabil. 1986; 13:169–81. DOI: 10.1111/j.1365-2842.1986.tb00649.x. PMID: 3457134.3. Rugh JD, Drago CJ. Vertical dimension: a study of clinical rest position and jaw muscle activity. J Prosthet Dent. 1981; 45:670–5. DOI: 10.1016/0022-3913(81)90426-1.4. Fayz F, Eslami A. Determination of occlusal vertical dimension: a literature review. J Prosthet Dent. 1988; 59:321–3. DOI: 10.1016/0022-3913(88)90182-5.5. Dawson PE. Functional occlusion from TMJ to smile design. 2007. 1st ed. New York: Elsevier Inc;p. 114–9.6. Mack MR. Vertical dimension: a dynamic concept based on facial form and oropharyngeal function. J Prosthet Dent. 1991; 66:478–85. DOI: 10.1016/0022-3913(91)90508-T.7. Jensen WO. Occlusion for the Class II jaw relations patient. J Prosthet Dent. 1990; 64:432–4. DOI: 10.1016/0022-3913(90)90039-F.8. Wassell RW, Steele JG, Welsh G. Considerations when planning occlusal rehabilitation: a review of the literature. Int Dent J. 1998; 48:571–81. DOI: 10.1111/j.1875-595X.1998.tb00494.x. PMID: 9881291.9. Kobayashi Y, Shibuya H, Nagano T, Yanagita S. Treatment of the temporomandibular joint dysfunction patient by full mouth occlusal reconstruction (author’s transl). Shigaku. 1975; 63:79–93. PMID: 1074044.10. Bloom DR, Padayachy JN. Increasing occlusal vertical dimension-why, when and how. Br Dent J. 2006; 200:251–6. DOI: 10.1038/sj.bdj.4813305. PMID: 16528325.11. Aboul-Ela LM, Razek MK. Pre-extraction records of the occlusal plane and vertical dimension. J Prosthet Dent. 1977; 38:490–3. DOI: 10.1016/0022-3913(77)90023-3.12. Mack MR. Perspective of facial esthetics in dental treatment planning. J Prosthet Dent. 1996; 75:16976. DOI: 10.1016/S0022-3913(96)90095-5.13. Willis FM. Features of the face involved in full denture prosthesis. Dent Cosmos. 1935; 77:851–54.14. Abduo J, Lyons K. Clinical considerations for increasing occlusal vertical dimension: a review. Aust Dent J. 2012; 57:2–10. DOI: 10.1111/j.1834-7819.2011.01640.x. PMID: 22369551.15. Turner KA, Missirlian DM. Restoration of the extremely worn dentition. J Prosthet Dent. 1984; 52:467–74. DOI: 10.1016/0022-3913(84)90326-3.16. Williamson EH, Lundquist DO. Anterior guidance: its effect on electromyographic activity of the temporal and masseter muscles. J Prosthet Dent. 1983; 49:816–23. DOI: 10.1016/0022-3913(83)90356-6.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Full mouth rehabilitation on the patient with deep bite and posterior bite collapse using re-establishment of occlusal vertical dimension
- Full mouth rehabilitation of patient with decreased occlusal vertical dimension due to severely worn dentition and posterior bite collapse
- The evaluation of maximum bite force in the occlusal rehabilitation of patient with Angle Class III malocclusion: a case report
- Full mouth rehabilitation in patient with deep bite, inter-dental arch discrepancy and loss of vertical dimension: a case report
- Full mouth rehabilitation in patient with loss of vertical dimension and deep bite due to tooth wear
