Vanishing Left Ventricular Thrombi in Severe Aortic Stenosis with Dilated Cardiomyopathy
- Affiliations
-
- 1Department of Cardiology, King Georges' Medical University, Lucknow, India. dr.rajivkharwar@gmail.com
- KMID: 2177472
- DOI: http://doi.org/10.4250/jcu.2014.22.2.98
Abstract
- No abstract available.
Figure
-

Fig. 1 Two dimensional transthoracic echocardiography with color Doppler. Multiple large layered as well as non-layered thrombi in LV marked by * are seen in slightly tilted parasternal long axis view (A) and in short axis view at the papillary muscle level (B). Bicuspid AV is clearly visible in parasternal basal short axis view (C) which was the cause of severe aortic stenosis with a peak velocity of 4.2 m/s on continuous wave Doppler (D). AV: aortic valve, LA: left atrium, LV: left ventricle, RA: right atrium, RV: right ventricle.
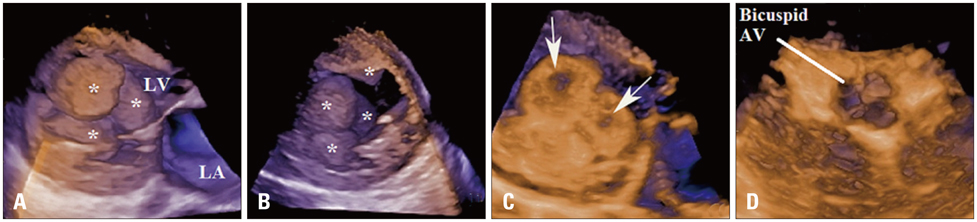
Fig. 2 Real time three dimensional transthoracic echocardiography with volume rendering. The size, shape, number, mobility, surface characteristics, intracardiac location of thrombi can be clearly delineated in various imaging planes (A and B). Echolucency within the thrombi (arrows in C) is seen suggestive of clot lysis beginning from inside to outside. Bicuspid AV can be delineated in three dimensional full volume zoomed mode (D). Thrombi in LV are marked by *. AV: aortic valve, LA: left atrium, LV: left ventricle.

Fig. 3 Two dimensional transthoracic echocardiography after 8 weeks of anticoagulation therapy. The multiple thrombi in the LV cavity have completely disappeared as seen in apical four chamber (A), parasternal long (B), and short axis (C) views. The LV ejection fraction is 25% which has relatively unchanged from the previous reading (D). Ao: aorta, LA: left atrium, LV: left ventricle, RA: right atrium, RV: right ventricle.
Reference
-
1. Nistri S, Basso C, Marzari C, Mormino P, Thiene G. Frequency of bicuspid aortic valve in young male conscripts by echocardiogram. Am J Cardiol. 2005; 96:718–721.
Article2. Gottdiener JS, Gay JA, VanVoorhees L, DiBianco R, Fletcher RD. Frequency and embolic potential of left ventricular thrombus in dilated cardiomyopathy: assessment by 2-dimensional echocardiography. Am J Cardiol. 1983; 52:1281–1285.
Article3. Visser CA, Kan G, David GK, Lie KI, Durrer D. Two dimensional echocardiography in the diagnosis of left ventricular thrombus. A prospective study of 67 patients with anatomic validation. Chest. 1983; 83:228–232.
Article4. Duncan K, Nanda NC, Foster WA, Mehmood F, Patel V, Singh A. Incremental value of live/real time three-dimensional transthoracic echocardiography in the assessment of left ventricular thrombi. Echocardiography. 2006; 23:68–72.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hemodynamics and Left Ventricular Cineangiographic Findings in Idiopathic Dilated Cardiomyopathy
- A Study of Left Ventricular Function by Digitized Echocardiograms in Dilated Cardiomyopathy
- Multiplane Transesophageal Echocardiographic Findings of Two Cases of Discrete Subvalvular Aortic Stenosis
- Echocardiographic Measurement of Systolic Time Intervals in Normal Adults and the Patients with Dilated Cardiomyopathy
- A Case of Normalized Hypertrophic Cardiomyopathy after Removal of Pheochromocytoma
