J Adv Prosthodont.
2012 Nov;4(4):235-238. 10.4047/jap.2012.4.4.235.
Magnet retained intraoral-extra oral combination prosthesis: a case report
- Affiliations
-
- 1Awadh Dental College & Hospital, Jamshedpur, India. sauravbnrj@gmail.com
- 2IDEAS, Gwalior, Madhya Pradesh, India.
- 3Dr R Ahmed Dental College & Hospital, Kolkata, India.
- 4Kalinga Institute of Dental Sciences, Bhubaneswar, India.
- KMID: 2176423
- DOI: http://doi.org/10.4047/jap.2012.4.4.235
Abstract
- Facial prosthesis is generally considered over surgical reconstruction to restore function and appearance in patients with facial defects that resulted from cancer resection. Retention of the prosthesis is challenging due to its size and weight. Retention can be achieved by using medical grade adhesives, resilient attachments, clips and osseointegrated implants. It can also be connected to obturator by magnets. This clinical report highlights the rehabilitation of a lateral midfacial defect with a two piece prosthesis that included an extra oral facial prosthesis and an intraoral obturator with the use of magnets.
Figure
-
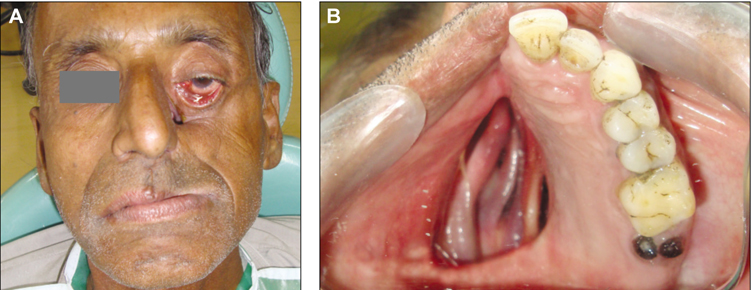
Fig. 1 A: Preoperative extra oral frontal view, B: Preoperative intraoral view (mirror view).

Fig. 2 Facial moulage impression made with irreversible hydrocolloid impression material.

Fig. 3 Postoperative extra oral frontal view with prosthesis.

Fig. 4 A: Procedure for making the prosthesis hollow using putty consistency poly (vinyl siloxane), B: Procedure for making the prosthesis hollow using salt.

Fig. 5 Intraoral obturator prosthesis with magnet.

Fig. 6 Intraoral obturator prosthesis (mirror view).

Fig. 7 Intraoral prosthesis attached to extra oral prosthesis.
Reference
-
1. Marunick MT, Harrison R, Beumer J 3rd. Prosthodontic rehabilitation of midfacial defects. J Prosthet Dent. 1985. 54:553–560.2. Guttal SS, Patil NP, Shetye AD. Prosthetic rehabilitation of a midfacial defect resulting from lethal midline granuloma-a clinical report. J Oral Rehabil. 2006. 33:863–867.3. Cowan PW. An obturator prosthesis. Quintessence Int. 1985. 16:403–405.4. Sykes LM, Essop RM. Combination intraoral and extraoral prosthesis used for rehabilitation of a patient treated for cancrum oris: a clinical report. J Prosthet Dent. 2000. 83:613–616.5. Thomas K. Prosthetic rehabilitation. 1994. London: Quintessence Publishing;93–103.6. Menneking H, Klein M, Hell B, Bier J. Prosthetic restoration of nasal defects: Indications for two different osseointegrated implant systems. J Facial Somato Prosthet. 1998. 4:29–33.7. Worthington P, Bränemark PI. Advanced osseointegration surgery applications in the maxillofacial region. 1992. Carol Stream, Il: Quintessence;307–326.8. Drago CJ. Tarnish and corrosion with the use of intraoral magnets. J Prosthet Dent. 1991. 66:536–540.9. Arcuri MR, LaVelle WE, Fyler E, Jons R. Prosthetic complications of extraoral implants. J Prosthet Dent. 1993. 69:289–292.10. Roumanas E, Nishumura R, Beumer J, Moy P, Weinlander M, Lorant J. Osseointegrated implants: Six-year follow-up report on the success rates of craniofacial implants at UCLA. Int J Oral Maxillofac Implants. 1994. 9:579–585.11. Patil PG. Modified technique to fabricate a hollow light-weight facial prosthesis for lateral midfacial defect: a clinical report. J Adv Prosthodont. 2010. 2:65–70.12. Matalon V, LaFuente H. A simplified method for making a hollow obturator. J Prosthet Dent. 1976. 36:580–582.13. Schneider A. Method of fabricating a hollow bulb obturator. J Prosthet Dent. 1978. 40:351.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Reconstruction of External Ear with Bone-Anchored Auricular Prosthesis: A Case Report and Literature Review
- Modified technique to fabricate a hollow light-weight facial prosthesis for lateral midfacial defect: a clinical report
- Axial displacement in single-tooth implant restoration: Case report
- Implant prosthesis using intraoral scanner: Case Report
- Fixed implant rehabilitation of maxillary edentulous patient using intraoral scanning digital workflow: a case report
