Multiple Symmetric Lipomatosis (Madelung's Disease) Presenting as Bilateral Huge Gynecomastia
- Affiliations
-
- 1Department of Medicine, Graduate School, Kyung Hee University, Seoul, Korea.
- 2Department of Surgery, Kyung Hee University Hospital at Gangdong, Kyung Hee University School of Medicine, Seoul, Korea. jeonguni@khu.ac.kr
- 3Department of Radiology, Kyung Hee University Hospital at Gangdong, Kyung Hee University School of Medicine, Seoul, Korea.
- KMID: 2176133
- DOI: http://doi.org/10.4048/jbc.2014.17.4.397
Abstract
- Multiple symmetric lipomatosis (MSL), or Madelung's disease, is a rare disease of unknown etiology. It is characterized by the presence of loose adipose tissue deposits localized in the cervical region and upper body. MSL presenting as bilateral huge gynecomastia is an extremely rare phenomenon. The present report describes a case of MSL in a 66-year-old man. The patients presented with bilateral breast bulging. He had a history of cigarette and alcohol use. His condition was treated with a bilateral nipple-sparing mastectomy. MSL can present as a form of gynecomastia, for its accurate diagnosis and proper treatment of MSL, increasing awareness of the clinical characteristics of the disease is required, especially amongst breast surgeons. Herein, we review the literature and discuss the clinical characteristics, pathology, and surgical treatment of MSL.
MeSH Terms
Figure
-
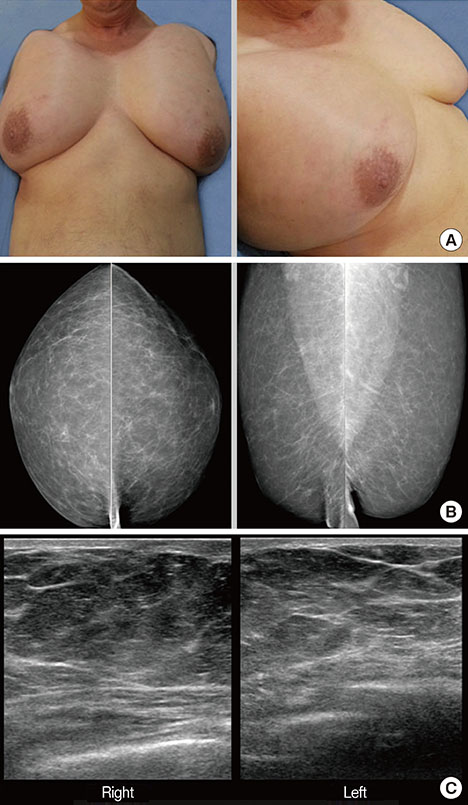
Figure 1 Physical findings and imaging studies of the patient. (A) Breast masses had elastic consistency and could be moved without causing any pain. Mammography (B) and ultrasonography (C) shows bilateral excessive fatty breast without definite glandular tissue (pseudogynecomastia).
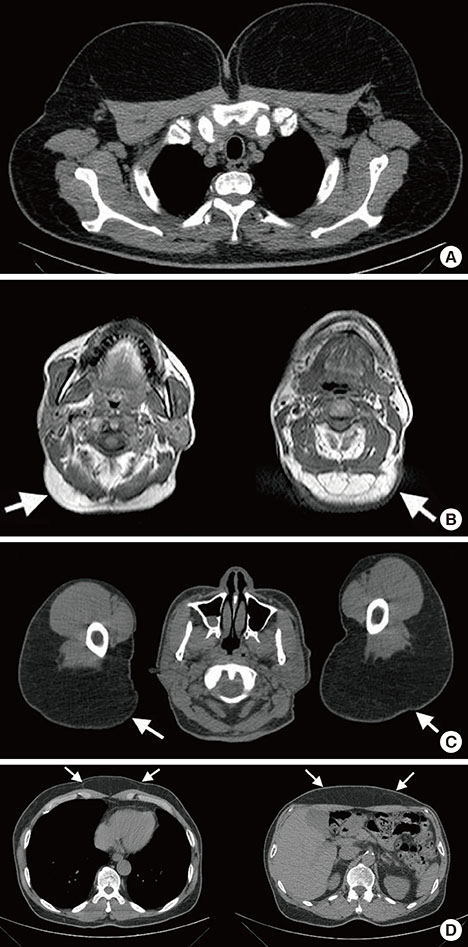
Figure 2 Computed tomography (CT) and magnetic resonance imaging (MRI) findings of the patient. (A) Marked bulging contours of both breasts with fat depositions are observed on CT scan. (B) MRI shows fat deposition in occipital lesion (white arrow). (C) CT scan shows bilateral fat deposition in shoulder (white arrow). (D) Excessive focal fat deposition as another focus of lipoma is also observed in superficial soft tissue layer of upper central abdomen on CT scan (white arrow).

Figure 3 Postoperative physical finding and breast specimen. (A) The patient underwent both nipple-sparing mastectomy with nipple interposition. (B) Breast specimen shows multiple lipomas, which were measured 30×17×5 cm (right) and 27×16×5 cm (left), respectively.

Figure 4 Microscopic pictures of specimen. Diffuse proliferation of normal adipose tissue is observed in microscopic pictures of specimen (H&E stain, ×100).
Reference
-
1. Ardeleanu V, Chicos S, Georgescu C, Tutunaru D. Multiple benign symmetric lipomatosis: a differential diagnosis of obesity. Chirurgia (Bucur). 2013; 108:580–583.2. Meningaud JP, Pitak-Arnnop P, Bertrand JC. Multiple symmetric lipomatosis: case report and review of the literature. J Oral Maxillofac Surg. 2007; 65:1365–1369.
Article3. Lopez-Ceres A, Aguilar-Lizarralde Y, Villalobos Sánchez A, Prieto Sánchez E, Valiente Alvarez A. Benign symmetric lipomatosis of the tongue in Madelung's disease. J Craniomaxillofac Surg. 2006; 34:489–493.
Article4. Donhauser G, Vieluf D, Ruzicka T, Braun-Falco O. Benign symmetric Launois-Bensaude type III lipomatosis and Bureau-Barrière syndrome. Hautarzt. 1991; 42:311–314.5. Mevio E, Sbrocca M, Mullace M, Viglione S, Mevio N. Multiple symmetric lipomatosis: a review of 3 cases. Case Rep Otolaryngol. 2012; 2012:910526.
Article6. Enzi G. Multiple symmetric lipomatosis: an updated clinical report. Medicine (Baltimore). 1984; 63:56–64.7. Brea-García B, Cameselle-Teijeiro J, Couto-González I, Taboada-Suárez A, González-Álvarez E. Madelung's disease: comorbidities, fatty mass distribution, and response to treatment of 22 patients. Aesthetic Plast Surg. 2013; 37:409–416.
Article8. Busetto L, Sträter D, Enzi G, Coin A, Sergi G, Inelmen EM, et al. Differential clinical expression of multiple symmetric lipomatosis in men and women. Int J Obes Relat Metab Disord. 2003; 27:1419–1422.
Article9. Borriello M, Lucidi A, Carbone A, Iannone V, Ferrandina G. Malignant transformation of Madelung's disease in a patient with a coincidental diagnosis of breast cancer: a case report. Diagn Pathol. 2012; 7:116.
Article10. Tizian C, Berger A, Vykoupil KF. Malignant degeneration in Madelung's disease (benign lipomatosis of the neck): case report. Br J Plast Surg. 1983; 36:187–189.
Article11. Plummer C, Spring PJ, Marotta R, Chin J, Taylor G, Sharpe D, et al. Multiple symmetrical lipomatosis: a mitochondrial disorder of brown fat. Mitochondrion. 2013; 13:269–276.
Article12. Heike Z, Gudrun UM, Frank RD, Vetter H, Walger P. Multiple benign symmetric lipomatosis: a differential diagnosis of obesity: is there a rationale for fibrate treatment? Obes Surg. 2008; 18:240–242.
Article13. Verhelle NA, Nizet JL, Van den Hof B, Guelinckx P, Heymans O. Liposuction in benign symmetric lipomatosis: sense or senseless? Aesthetic Plast Surg. 2003; 27:319–321.
Article
