J Korean Diabetes.
2014 Sep;15(3):142-145. 10.4093/jkd.2014.15.3.142.
The Role of the Kidney in Glucose Metabolism
- Affiliations
-
- 1Department of Endocrinology and Metabolism, Kyung Hee University School of Medicine, Seoul, Korea. bard95@hanmail.net
- KMID: 2173884
- DOI: http://doi.org/10.4093/jkd.2014.15.3.142
Abstract
- It is well known that the kidney is important for maintaining glucose homeostasis in vivo. However, the physiological role of the kidney in glucose metabolism is typically underestimated. Recently, a new class of anti-diabetic medications that affect the renal glucose regulatory mechanism was introduced into the market, sparking the interest of many researchers to better understand this mechanism. In this article, I briefly describe the role of the kidney in glucose metabolism and the changes of its function in patients with diabetes mellitus.
MeSH Terms
Figure
-
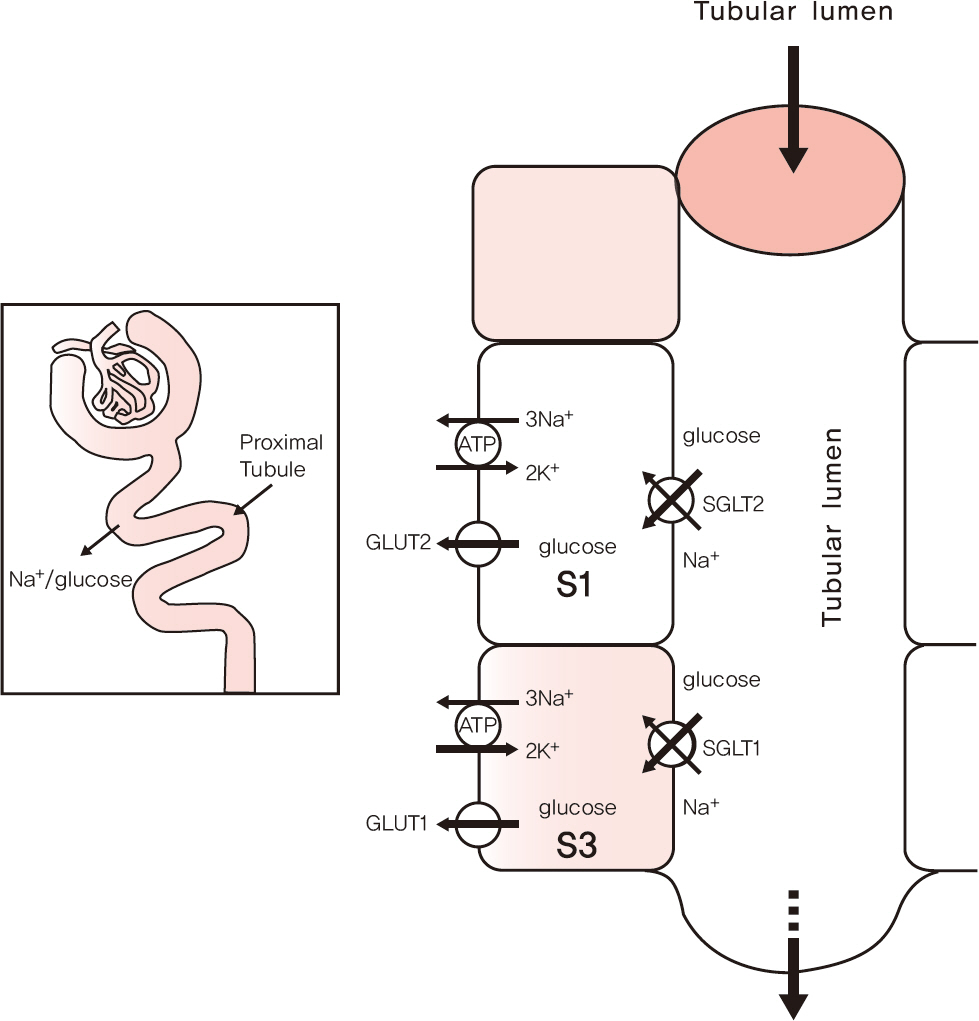
Fig. 1. Sodium glucose cotransporters (SGLTs) in the kidney. Adapted from Santer R, et al. Clin J Am Soc Nephrol 2010;5:133-41[12].
Reference
-
1. Abdul-Ghani MA, Norton L, Defronzo RA. Role of sodiumglucose cotransporter 2 (SGLT 2) inhibitors in the treatment of type 2 diabetes. Endocr Rev. 2011; 32:515–31.
Article2. Holt RI, Cockram C, Flyvbjerg A, Goldstein BJ. Goldstein Textbook of Diabetes. 4th ed.Hoboken: Wiley-Blackwell;2010.3. Gerich JE. Role of the kidney in normal glucose homeostasis and in thehyperglycaemia of diabetes mellitus: therapeutic implications. Diabet Med. 2010; 27:136–42.4. Gerich JE. Physiology of glucose homeostasis. Diabetes ObesMetab. 2000; 2:345–50.
Article5. Stumvoll M, Meyer C, Mitrakou A, Nadkarni V, Gerich JE. Renal glucoseproduction and utilization: new aspects in humans. Diabetologia. 1997; 40:749–57.6. Meyer C, Dostou JM, Welle SL, Gerich JE. Role of human liver, kidney, andskeletal muscle in postprandial glucose homeostasis. Am J PhysiolEndocrinolMetab. 2002; 282:E419–27.7. Stumvoll M, Meyer C, Perriello G, Kreider M, Welle S, Gerich J. Human kidneyand liver gluconeogenesis: evidence for organ substrate selectivity. Am JPhysiol. 1998; 274(5 Pt 1):E817–26.8. Meyer C, Dostou JM, Gerich JE. Role of the human kidney in glucosecounterregulation. Diabetes. 1999; 48:943–8.9. Gerich JE. Hepatorenal glucose reciprocity in physiologic and pathologicconditions. Diabetes NutrMetab. 2002; 15:298–302.10. Brown GK. Glucose transporters: structure, function and consequences ofdeficiency. J Inherit Metab Dis. 2000; 23:237–46.11. Wright EM, Hirayama BA, Loo DF. Active sugar transport in health and disease.J Intern Med. 2007; 261:32–43.12. Santer R, Calado J. Familial renal glucosuria and SGLT2: from a mendeliantrait to a therapeutic target. Clin J Am SocNephrol. 2010; 5:133–41.13. Johansen K, Svendsen PA, L⊘rup B. Variations in renal threshold for glucosein Type 1 (insulin-dependent) diabetes mellitus. Diabetologia. 1984; 26:180–2.
Article14. Wright EM. Renal Na(+)-glucose cotransporters. Am J Physiol Renal Physiol. 2001; 280:F10–8.
Article15. Hediger MA, Rhoads DB. Molecular physiology of sodiumglucose cotransporters. Physiol Rev. 1994; 74:993–1026.16. Santer R, Kinner M, Lassen CL, Schneppenheim R, Eggert P, Bald M, Brodehl J, Daschner M, Ehrich JH, Kemper M, Li Volti S, Neuhaus T, Skovby F, Swift PG, Schaub J, Klaerke D. Molecular analysis of the SGLT2 gene in patients with renal glucosuria. J AmSocNephrol. 2003; 14:2873–82.
Article17. Meyer C, Stumvoll M, Nadkarni V, Dostou J, Mitrakou A, Gerich J. Abnormalrenal and hepatic glucose metabolism in type 2 diabetes mellitus. J Clin Invest. 1998; 102:619–24.18. Meyer C, Woerle HJ, Dostou JM, Welle SL, Gerich JE. Abnormal renal, hepatic, and muscle glucose metabolism following glucose ingestion in type 2 diabetes. Am J PhysiolEndocrinolMetab. 2004; 287:E1049–56.
Article19. Landau BR. Gluconeogenesis and pyruvate metabolism in rat kidney, in vitro. Endocrinology. 1960; 67:744–51.20. Krebs HA, Speake RN, Hems R. Acceleration of renal gluconeogenesis by ketone bodies and fatty acids. Biochem J. 1965; 94:712–20.
Article21. Williamson JR. Mechanism for the stimulation in vivo of hepaticgluconeogenesis by glucagon. Biochem J. 1966; 101:11C–14C.22. Wolf S, Rave K, Heinemann L, Roggen K. Renal glucose excretion and tubularreabsorption rate related to blood glucose in subjects with type 2 diabetes with a critical reappraisal of the "renal glucose threshold" model. Horm Metab Res. 2009; 41:600–4.23. Mogensen CE. Maximum tubular reabsorption capacity for glucose and renalhemodynamcis during rapid hypertonic glucose infusion in normal and diabeticsubjects. Scand J Clin Lab Invest. 1971; 28:101–9.24. Rahmoune H, Thompson PW, Ward JM, Smith CD, Hong G, Brown J. Glucosetransporters in human renal proximal tubular cells isolated from the urine ofpatients with non-insulin-dependent diabetes. Diabetes. 2005; 54:3427–34.25. Vestri S, Okamoto MM, de Freitas HS, Aparecida Dos Santos R, Nunes MT, Morimatsu M, Heimann JC, Machado UF. Changes in sodium or glucose filtration ratemodulate expression of glucose transporters in renal proximal tubular cells ofrat. J MembrBiol. 2001; 182:105–12.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Sodium-Glucose Cotransporter 2 Inhibitors: Mechanisms of Action and Various Effects
- Emerging role of the brain in the homeostatic regulation of energy and glucose metabolism
- A study on Glucose Metabolism in Newborn Infants
- The Impaired Glucose Metabolism in Patients with Cushing's Syndrome
- The Genes of Hepatic Glucose Metabolism and Insulin Signaling
