Chonnam Med J.
2008 Dec;44(3):125-131. 10.4068/cmj.2008.44.3.125.
Anterior Thoracolumbar Fusion with Titanium Mesh Cage
- Affiliations
-
- 1Department of Neurosurgery, Chonnam National University Hospital and Medical School, Gwangju, Korea. stylish74@hanmail.net
- 2Department of Neurosurgery, Seonam University Nam-Gwang Hospital, Gwangju, Korea.
- KMID: 2172290
- DOI: http://doi.org/10.4068/cmj.2008.44.3.125
Abstract
- Destructions of vertebral body due to various medical situations including acute fracture, tumor, post-traumatic deformity and infection lead to progressive destruction of vertebral body, kyphotic deformities and further neurological defecits. Titanium mesh cages (TMCs) with cancellous autograft bone after corpectomy of the thoracolumbar spine provide immediate structural support to the anterior column. The aim of this study was to evaluate the radiological, neurological and clinical outcomes of the patients with the TMCs-bone graft composite after thoracolumbar corpectomy. Sixteen patients underwent reconstruction using titanium mesh cages in thoracolumbar corpectomy between July 2000 and February 2005. The radiological and clinical course was documented over a mean follow-up duration of 28.2 months. The degree of kyphosis, construct height and the subsidence of the cage in relation to the vertebral endplates were measured preoperatively, early postoperatively, and at the latest follow-up. The mean kyphotic angle of 3.9degrees before surgery was reduced to -2.6degrees immediately after surgery, and at the last follow-up to be 3.4degrees. There was a significant difference between the preoperative versus postoperative kyphotic angle (p=0.003). The mean construct height of the involved vertebrae before surgery was 41.6 mm and the mean construct height immediate after surgery and at follow-up were 47.9 and 41.5 mm, respectively. There was a significant difference between the preoperative versus postoperative construct height (p<0.0001). But there was no significant difference between the preoperative versus follow-up in kyphotic angle and construct height. The mean subsidence was 5.7 mm. However, there was no case of severe collapse or significant recurrence of deformity. In no patients, significant neurological deterioration was detected after surgery, and neither with major complications. This study demonstrated that TMCs after thoracolumbar corpectomy is a successful adjunct for anterior vertebral column reconstruction. In our cases, TMCs with anterior instrumentation allows a good structural support and maintain spinal alignment.
MeSH Terms
Figure
-

Fig. 1 Illustration for Cobb angle measurement.
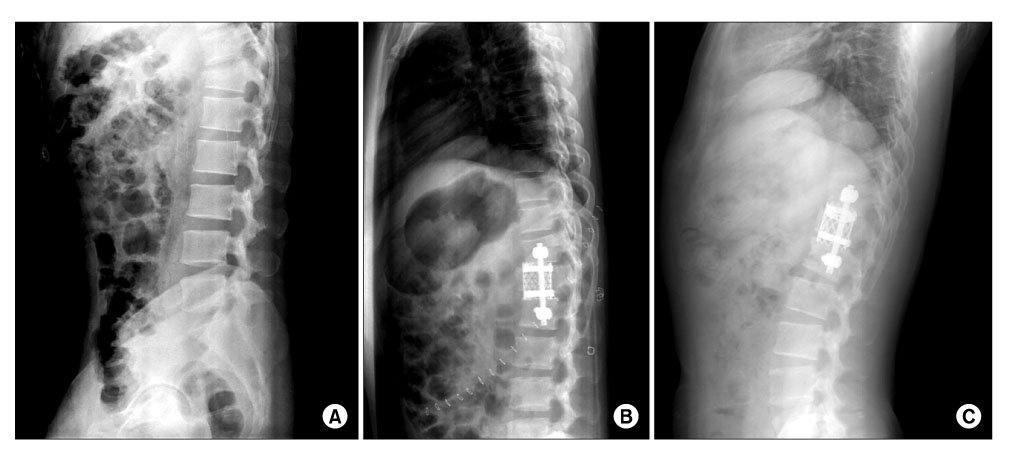
Fig. 2 Preoperative (A), early postoperative (B) and 14 months (C) follow-up lateral radiographs of a 29-years-old man with T12 burst fracture treated with titanium mesh cage with single screw and rod system after corpectomy.
Reference
-
1. Blumenthal SL, Gill K. Can lumbar spine radiographs accurately determine fusion in postoperative patients? Correlation of routine radiographs with a second surgical look at lumbar fusions. Spine. 1993. 18:1186–1189.
Article2. Bridwell KH, Lenke LG, McEnery KW, Baldus C, Blanke K. Anterior fresh frozen structural allografts in the thoracic and lumbar spine. Do they work if combined with posterior fusion and instrumentation in adult patients with kyphosis or anterior column defects? Spine. 1995. 20:1410–1418.
Article3. Finkelstein JA, Chapman JR, Mirza S. Anterior cortical allograft in thoracolumbar fractures. J Spinal Disord. 1999. 12:424–429.
Article4. Hussein AA, El-Karef E, Hafez M. Reconstructive surgery in spinal tumors. Eur J Surg Oncol. 2001. 27:196–199.5. Sasso RC, Best NM, Reilly TM, McGuire RA Jr. Anterior-only stabilization of three- column thoracolumbar injuries. J Spinal Disord Tech. 2005. 18:Suppl. S7–S14.6. Kostuik JP. Anterior fixation for fractures of the thoracic and lumbar spine with or without neurologic involvement. Clin Orthop Relat Res. 1984. 189:103–115.
Article7. Dvorak MF, Kwon BK, Fisher CG, Eiserloh HL 3rd, Boyd M, Wing PC. Effectiveness of titanium mesh cylindrical cages in anterior column reconstruction after thoracic and lumbar vertebral body resection. Spine. 2003. 28:902–908.
Article8. Robertson PA, Rawlinson HJ, Hadlow AT. Radiologic stability of titanium mesh cages for anterior spinal reconstruction following thoracolumbar corpectomy. J Spinal Disord Tech. 2004. 17:44–52.
Article9. Hong JT, Lee SW, Son BC, Sung JH, Park CK, Kim MC. Kyphotic angle measurement accuracy for vertebral osteoporotic compression fracture: reliable method for kyphotic angle measurement. J Korean Neurosurg Soc. 2006. 39:256–259.10. Roberson JR, Whitesides TE Jr. Surgical reconstruction of late post-traumatic thoracolumbar kyphosis. Spine. 1985. 10:307–312.
Article11. Streitz W, Brown JC, Bonnett CA. Anterior fibular strut grafting in the treatment of kyphosis. Clin Orthop Relat Res. 1977. 128:140–148.
Article12. Eck KR, Bridwell KH, Ungacta FF, Lapp MA, Lenke LG, Riew KD. Analysis of titanium mesh cages in adults with minimum two-year follow-up. Spine. 2000. 25:2407–2415.
Article13. Molinari RW, Bridwell KH, Klepps SJ, Baldus C. Minimum 5-year follow-up of anterior column structural allografts in the thoracic and lumbar spine. Spine. 1999. 24:967–972.
Article14. Singh K, DeWald CJ, Hammerberg KW, DeWald RL. Long structural allografts in the treatment of anterior spinal column defects. Clin Orthop Relat Res. 2002. 394:121–129.
Article15. Lee SW, Lim TH, You JW, An HS. Biomechanical effect of anterior grafting devices on the rotational stability of spinal constructs. J Spinal Disord. 2000. 13:150–155.
Article16. Vahldiek MJ, Panjabi MM. Stability potential of spinal instrumentations in tumor vertebral body replacement surgery. Spine. 1998. 23:543–550.
Article17. Hasegawa K, Abe M, Washio T, Hara T. An experimental study on the interface strength between titanium mesh cage and vertebra in reference to vertebral bone mineral density. Spine. 2001. 26:957–963.
Article18. Schnee CL, Ansell LV. Selection criteria and outcome of operative approaches for thoracolumbar burst fractures with and without neurological deficit. J Neurosurg. 1997. 86:48–55.
Article19. Brodke DS, Gollogly S, Bachus KN, Alexander Mohr R, Nguyen BK. Anterior thoracolumbar instrumentation: stiffness and load sharing characteristics of plate and rod systems. Spine. 2003. 28:1794–1801.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Efficacy of Titanium Mesh Cage in Tuberculous Spondylitis Treated with Anterior Intervertebral Fusion
- Result of anterior Decompression and Stabilization with KANEDA II Device and SURGICAL TITANIUM MESH in Thoracolumbar Unstble Spine Injuries
- Titanium Mesh Cage for Anterior Stabilization in Tuberculous Spondylitis : Is It Safe?
- Efficacy of Titanium Mesh Cages for Anterior Column Reconstruction after Thoracolumbar Corpectomy
- The Advantages of Rectangular Titanium Cage(RABEA) Fusion after Anterior Cervical Discectomy: Comparative Study of Fibula Allograft
