A Latent Autoimmune Diabetes in Adults Patient Manifesting Severe Musculoskeletal Complications
- Affiliations
-
- 1Department of Endocrinology and Metabolism, Kyung Hee University College of Medicine, Seoul, Korea. imdrjs@khu.ac.kr
- KMID: 2170057
- DOI: http://doi.org/10.11005/jbm.2014.21.4.283
Abstract
- Patients with diabetes have many different kinds of complications involving multiple organs, but those involving the musculoskeletal system are relatively uncommon. Diabetic muscle infarction (DMI) is a rare, painful, and potentially serious condition in patients with poorly controlled diabetes mellitus. A 35-year-old man diagnosed with type 2 diabetes eight years ago, visited with severe muscle pain in the right anteromedial thigh without any event of trauma. He had been treated with metformin, but his glycemic control was very poor with a glycated hemoglobin of 14.5%. Evaluation of his painful thigh lesion did not reveal any evidence of infection or vasculitis, but the magnetic resonance imaging and bone scan showed findings of DMI at vastus medialis muscle and an insufficiency fracture at the right medial tibial condyle. He was diagnosed with retinopathy, neuropathy and microalbuminuria but not macrovascular complications. We also diagnosed his diabetes as latent autoimmune diabetes in adults (LADA) based on his low C-peptide level, positive anti-glutamic acid decarboxylase (GAD) antibody and early onset diabetes. Instead of antibiotics, bed rest, analgesics and strict blood glucose control with multiple daily insulin injections led to symptom improvement. This is an unusual case of a young man with LADA experiencing severe musculoskeletal complication of DMI and insufficiency fracture. If a poorly controlled diabetic patient appears to have unaccounted soft tissue pain, musculoskeletal complications such as DMI associated with hyperglycemia should be considered.
MeSH Terms
-
Adult*
Analgesics
Anti-Bacterial Agents
Bed Rest
Blood Glucose
C-Peptide
Diabetes Mellitus
Diabetes Mellitus, Type 1*
Fractures, Stress
Hemoglobin A, Glycosylated
Humans
Hyperglycemia
Infarction
Insulin
Magnetic Resonance Imaging
Metformin
Musculoskeletal System
Myalgia
Nociceptive Pain
Quadriceps Muscle
Thigh
Vasculitis
Analgesics
Anti-Bacterial Agents
Blood Glucose
C-Peptide
Insulin
Metformin
Figure
-
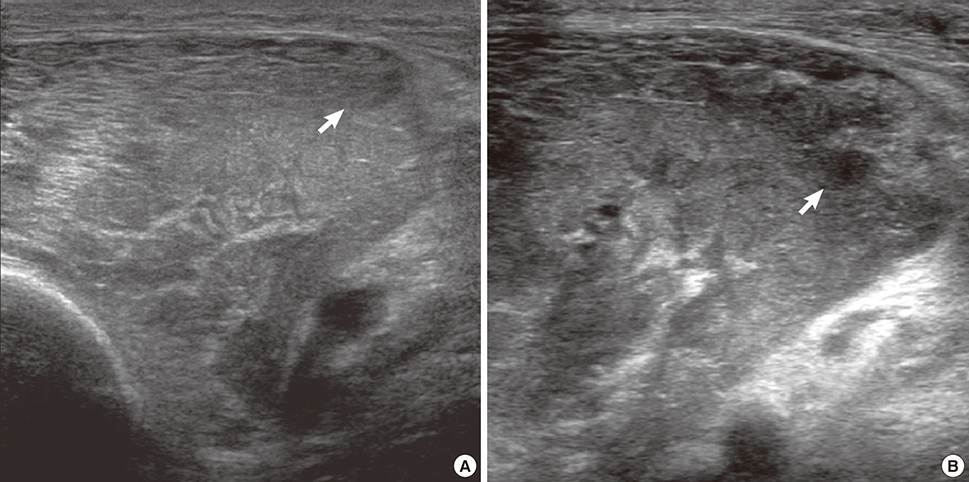
Fig. 1 Ultrasonography of the right thigh: (A) on admission, there was an ill-defined hyperechoic lesion and thick fluid collection (arrow) in the right vastus medialis. (B) After four days, there was an increase in the thick fluid collection (arrow) in the right vastus medialis.

Fig. 2 Magnetic resonance image (MRI) of the right thigh: (A) Fat-suppressed, gadolinium-enhanced T1 coronal MRI revealed diffuse enlargement of the vastus medialis muscle with a low signal area at the distal part, suggestive of partly decreased perfusion, and edematous change of the proximal part. The low signal lesion at the distal part of the muscle had irregularly linear, serpentine enhancing portions crossing the lesion and surrounding peripheral enhancement. Diffuse subcutaneous edema involving the entire thigh was seen. (B) On the fat-suppressed, gadolinium-enhanced T1 axial image scanned at the distal part of vastus medialis muscle, irregular dark signal foci (arrows) and intervening enhancing portions were seen within the low signal lesion. Note the ill-defined peripheral enhancement. (C) T2 axial image showed high signal intensity at the low signal lesion of the same part in (B).
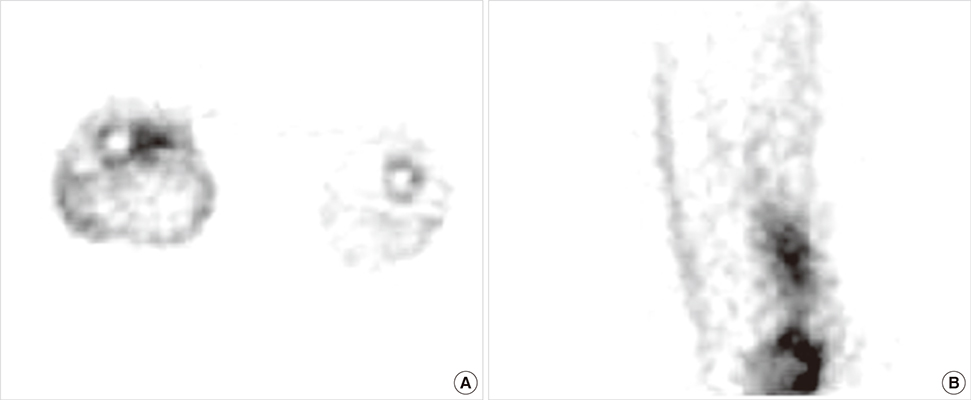
Fig. 3 (A) Cross-sectional view and (B) sagittal view of the three-phase bone scan: Increased perfusion, blood pool, and delayed uptake were seen at the right thigh, especially the lower medial portion of the right vastus medialis. This finding is consistent with myonecrosis as shown on the thigh magnetic resonance image.

Fig. 4 Insufficient fracture of the right knee on multiple imaging studies: (A) Three-phase bone scan, (B) simple X-ray, and (C) Coronal T1-weighted magnetic resonance image (MRI). MRI showed serpentine low-signaled line with surrounding ill-defined low signal area at the right medial tibial condyle, which is consistent with insufficient fracture with marrow edema.
Reference
-
1. Chason DP, Fleckenstein JL, Burns DK, et al. Diabetic muscle infarction: radiologic evaluation. Skeletal Radiol. 1996; 25:127–132.
Article2. Litvinov IV, Radu A, Garfield N. Diabetic muscle infarction in a 57 year old male: a case report. BMC Res Notes. 2012; 5:701.
Article3. Trujillo-Santos AJ. Diabetic muscle infarction: an underdiagnosed complication of long-standing diabetes. Diabetes Care. 2003; 26:211–215.4. Angervall L, Stener B. Tumoriform focal muscular degeneration in two diabetic patients. Diabetologia. 1965; 1:39–42.
Article5. Anderson WR, Richards AM. Evaluation of lower extremity muscle biopsies in the diagnosis of atheroembolism. Arch Pathol. 1968; 86:535–541.6. Said G, Lacroix C, Lozeron P, et al. Inflammatory vasculopathy in multifocal diabetic neuropathy. Brain. 2003; 126:376–385.
Article7. Atkinson MA, Maclaren NK. The pathogenesis of insulin-dependent diabetes mellitus. N Engl J Med. 1994; 331:1428–1436.
Article8. Betterle C, Zanette F, Pedini B, et al. Clinical and subclinical organ-specific autoimmune manifestations in type 1 (insulin-dependent) diabetic patients and their first-degree relatives. Diabetologia. 1984; 26:431–436.
Article9. Silberstein L, Britton KE, Marsh FP, et al. An unexpected cause of muscle pain in diabetes. Ann Rheum Dis. 2001; 60:310–312.
Article10. Gargiulo P, Schiaffini R, Bosco D, et al. Diabetic microangiopathy: lupus anticoagulant dependent thrombotic tendency in type 1 (insulin-dependent) diabetes mellitus. Diabet Med. 1997; 14:132–137.
Article11. Weissman J. Image interpretation session: 1996. Diabetic muscle infarction (DMI). Radiographics. 1997; 17:246–248.
Article12. Lafforgue P, Janand-Delenne B, Lassman-Vague V, et al. Painful swelling of the thigh in a diabetic patient: diabetic muscle infarction. Diabetes Metab. 1999; 25:255–260.13. Cernea S, Buzzetti R, Pozzilli P. Beta-cell protection and therapy for latent autoimmune diabetes in adults. Diabetes Care. 2009; 32:Suppl 2. S246–S252.14. Vestergaard P, Rejnmark L, Mosekilde L. Relative fracture risk in patients with diabetes mellitus, and the impact of insulin and oral antidiabetic medication on relative fracture risk. Diabetologia. 2005; 48:1292–1299.
Article15. Räkel A, Sheehy O, Rahme E, et al. Osteoporosis among patients with type 1 and type 2 diabetes. Diabetes Metab. 2008; 34:193–205.
Article16. Hofbauer LC, Brueck CC, Singh SK, et al. Osteoporosis in patients with diabetes mellitus. J Bone Miner Res. 2007; 22:1317–1328.
Article17. Patel S, Hyer S, Tweed K, et al. Risk factors for fractures and falls in older women with type 2 diabetes mellitus. Calcif Tissue Int. 2008; 82:87–91.
Article18. Holick MF. High prevalence of vitamin D inadequacy and implications for health. Mayo Clin Proc. 2006; 81:353–373.
Article19. Pittas AG, Lau J, Hu FB, et al. The role of vitamin D and calcium in type 2 diabetes. A systematic review and meta-analysis. J Clin Endocrinol Metab. 2007; 92:2017–2029.
Article20. Lemire JM. Immunomodulatory actions of 1,25-dihydroxyvitamin D3. J Steroid Biochem Mol Biol. 1995; 53:599–602.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Latent Autoimmune Diabetes in Adults: Autoimmune Diabetes in Adults with Slowly Progressive beta-cell Failure
- Latent Autoimmune Diabetes in Adults: Current Status and New Horizons
- Latent Autoimmune Diabetes in Adults: A Review on Clinical Implications and Management
- Musculoskeletal complications in patients with diabetes mellitus
- Clinical Heterogeneity of Diabetes in Young Korean Patients
