J Bone Metab.
2014 Nov;21(4):277-282. 10.11005/jbm.2014.21.4.277.
Mutiple Spontaneous Rib Fractures in Patient with Cushing's Syndrome
- Affiliations
-
- 1Division of Endocrinology and Metabolism, Department of Internal Medicine, College of Medicine, Korea University, Seoul, Korea. deisy21@naver.com
- KMID: 2170056
- DOI: http://doi.org/10.11005/jbm.2014.21.4.277
Abstract
- Glucocorticoid (GC) excess, including Cushing's syndrome, is a common cause of secondary osteoporosis. Thirty to fifty percent of Cushing's syndrome patients experience non-traumatic fractures, which is often the presenting manifestation of Cushing's syndrome. However, there have been rare cases of Cushing's syndrome diagnosed only based upon bone manifestations. We describe a case of Cushing's syndrome that was diagnosed in a 44-year-old woman who initially visited our hospital due to multiple non-traumatic rib fractures. She did not exhibit any other manifestations of Cushing's syndrome such as moon face, buffalo hump or abdominal striae. Initially, we evaluated her for bone metastases from a cancer of unknown origin, but there was no evidence of metastatic cancer. Instead, we found a left adrenal incidentaloma. As a result of the hormone study, she was diagnosed as having Cushing's syndrome. Interestingly, her bony manifestation of Cushing's syndrome, which was evident in the bone scan and bone mineral densitometry, completely recovered after a left adrenalectomy. Therefore, the possibility of Cushing's syndrome as a cause of secondary osteoporosis should be considered in young patients with non-traumatic multiple fractures, with or without any other typical features of Cushing's syndrome.
MeSH Terms
Figure
-

Fig. 1 Chest X-ray showed multiple sclerotic lesions of right 4th, 5th, 6th and 7th ribs.

Fig. 2 Chest computed tomography showed multiple sclerotic lesions of the ribs of both sides (left 4th, right 4th, 5th rib).
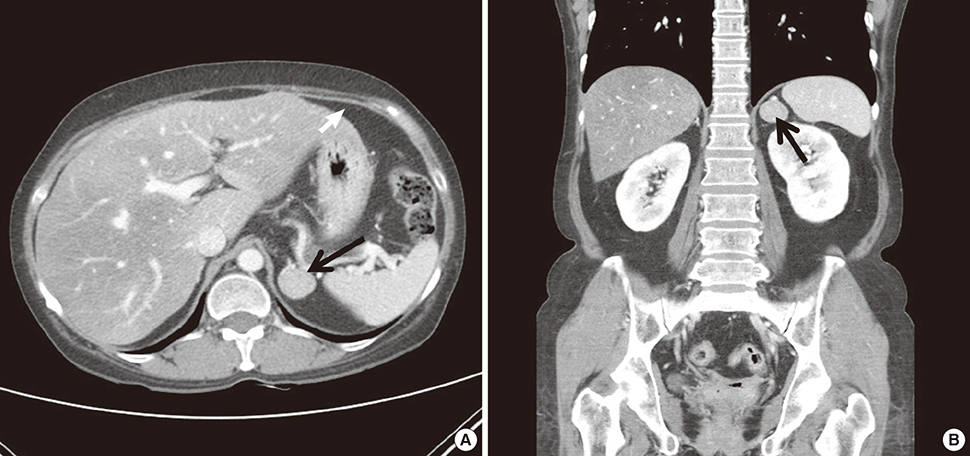
Fig. 3 Abdominal computed tomography showed a 2.5 × 2.0 cm sized mass (black arrow) on the left adrenal gland.
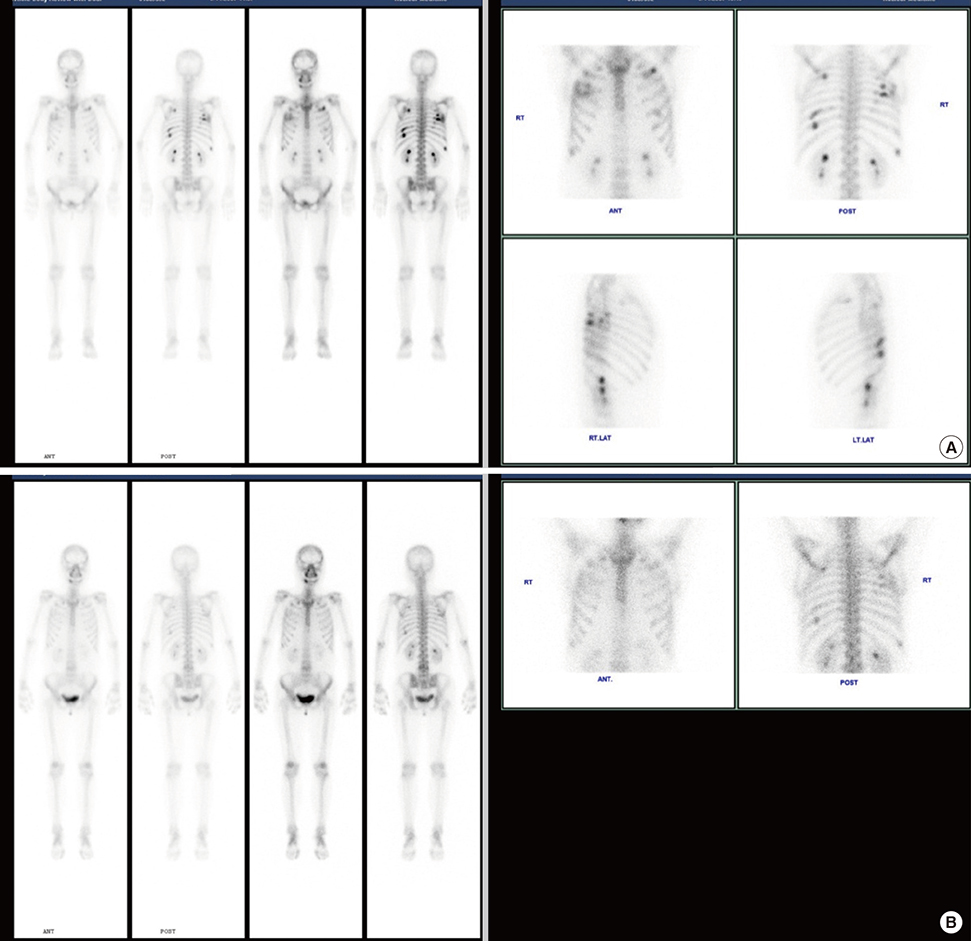
Fig. 4 (A) Bone scan showed multi-focal increased uptake in the ribs of both sides. (B) Multifocal uptakes are almost disappeared in the bilateral ribs 1 year after unilateral adrenalectomy.
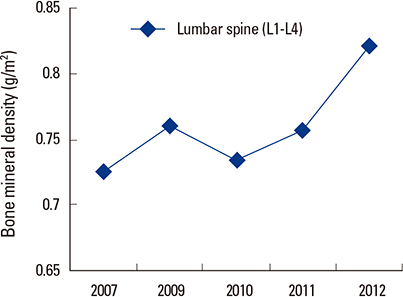
Fig. 5 The graph of her bone mineral density of the L1-L4 lumbar spine, which was improved gradually.
Reference
-
1. Hofbauer LC, Hamann C, Ebeling PR. Approach to the patient with secondary osteoporosis. Eur J Endocrinol. 2010; 162:1009–1020.
Article2. Tóth M, Grossman A. Glucocorticoid-induced osteoporosis: lessons from Cushing's syndrome. Clin Endocrinol (Oxf). 2013; 79:1–11.
Article3. Mancini T, Doga M, Mazziotti G, et al. Cushing's syndrome and bone. Pituitary. 2004; 7:249–252.
Article4. Kawamata A, Iihara M, Okamoto T, et al. Bone mineral density before and after surgical cure of Cushing's syndrome due to adrenocortical adenoma: prospective study. World J Surg. 2008; 32:890–896.
Article5. van der Eerden AW, den Heijer M, Oyen WJ, et al. Cushing's syndrome and bone mineral density: lowest Z scores in young patients. Neth J Med. 2007; 65:137–141.6. Arnaldi G, Angeli A, Atkinson AB, et al. Diagnosis and complications of Cushing's syndrome: a consensus statement. J Clin Endocrinol Metab. 2003; 88:5593–5602.
Article7. Han JY, Lee J, Kim GE, et al. A case of cushing syndrome diagnosed by recurrent pathologic fractures in a young woman. J Bone Metab. 2012; 19:153–158.
Article8. Jung MH, Choi H, Kim JY, et al. Vertebral compression fracture in Cushing's syndrome with adrenal adenoma. J Korean Soc Osteoporos. 2009; 7:209–213.9. Longo DL, Fauci AS, Kasper DL, et al. Harrison's principles of internal medicine. 18th ed. New York, NY: McGraw-Hill;2012.10. Boscaro M, Barzon L, Fallo F, et al. Cushing's syndrome. Lancet. 2001; 357:783–791.
Article11. Vestergaard P, Lindholm J, Jørgensen JO, et al. Increased risk of osteoporotic fractures in patients with Cushing's syndrome. Eur J Endocrinol. 2002; 146:51–56.
Article12. Camozzi V, Sanguin F, Albigier N, et al. Persistent increase of osteoprotegerin levels after cortisol normalization in patients with Cushing's syndrome. Eur J Endocrinol. 2010; 162:85–90.
Article13. Minetto M, Reimondo G, Osella G, et al. Bone loss is more severe in primary adrenal than in pituitary-dependent Cushing's syndrome. Osteoporos Int. 2004; 15:855–861.
Article14. Ohmori N, Nomura K, Ohmori K, et al. Osteoporosis is more prevalent in adrenal than in pituitary Cushing's syndrome. Endocr J. 2003; 50:1–7.
Article15. Mazziotti G, Angeli A, Bilezikian JP, et al. Glucocorticoid-induced osteoporosis: an update. Trends Endocrinol Metab. 2006; 17:144–149.
Article16. Canalis E. Clinical review 83: mechanisms of glucocorticoid action in bone: implications to glucocorticoid-induced osteoporosis. J Clin Endocrinol Metab. 1996; 81:3441–3447.
Article17. Manning PJ, Evans MC, Reid IR. Normal bone mineral density following cure of Cushing's syndrome. Clin Endocrinol (Oxf). 1992; 36:229–234.
Article18. Kristo C, Jemtland R, Ueland T, et al. Restoration of the coupling process and normalization of bone mass following successful treatment of endogenous Cushing's syndrome: a prospective, long-term study. Eur J Endocrinol. 2006; 154:109–118.
Article19. Luisetto G, Zangari M, Camozzi V, et al. Recovery of bone mineral density after surgical cure, but not by ketoconazole treatment, in Cushing's syndrome. Osteoporos Int. 2001; 12:956–960.
Article20. Di Somma C, Pivonello R, Loche S, et al. Effect of 2 years of cortisol normalization on the impaired bone mass and turnover in adolescent and adult patients with Cushing's disease: a prospective study. Clin Endocrinol (Oxf). 2003; 58:302–308.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Cushing Syndrome Diagnosed by Recurrent Pathologic Fractures in a Young Woman
- A Case of Cushing's Syndrome
- Rib Fractures: To Fix or Not to Fix? An Evidence-Based Algorithm
- A Case of Cushing's Syndrome caused by Adrenocortical Carcinoma
- Frequency of Multiple Consecutive Rib Fracture after Blunt Chest Trauma
