Anesth Pain Med.
2016 Jan;11(1):109-112. 10.17085/apm.2016.11.1.109.
Flexible bronchoscopic foreign body removal through the I-gel supraglottic airway: A case report
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Korea University Ansan Hospital, Ansan, Korea. yslee4719@gmail.com
- 2Department of Anesthesiology and Pain Medicine, Ajou Universitiy School of Medicine, Suwon, Korea.
- KMID: 2169085
- DOI: http://doi.org/10.17085/apm.2016.11.1.109
Abstract
- The daily insertion of endotracheal tubes, laryngeal mask airways, oral/nasal airways, gastric tubes, transesophageal echocardiogram probes, esophageal dilators and emergency airways all involve the risk of airway structure damage. In the closed claims analysis of the American Society of Anesthesiologists, 6% of all claims concerned airway injury. Among the airway injury clams, the most common cause was difficult intubation. Among many other causes, esophageal stethoscope is a relatively noninvasive monitor that provides extremely useful information. Relatively not many side effects that hardly is ratable. Some of that was from tracheal insertion, bronchial insertion resulting in hypoxia, hoarseness due to post cricoids inflammation, misguided surgical dissection of esophagus. Also oropharyngeal bleeding and subsequent anemia probably are possible and rarely pharyngeal/esophageal perforations are also possible because of this device. Careful and gentle procedure is necessary when inserting esophageal stethoscope and observations for injury and bleeding are needed after insertion.
Keyword
MeSH Terms
Figure
-
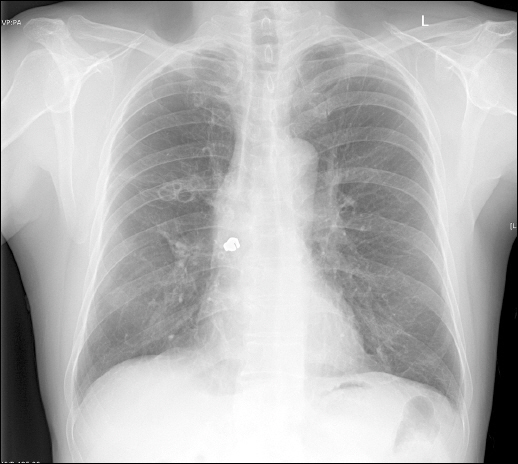
Fig. 1 Posteroanterior chest radiograph shows a radiopaque material lodged in the right bronchus intermedius.
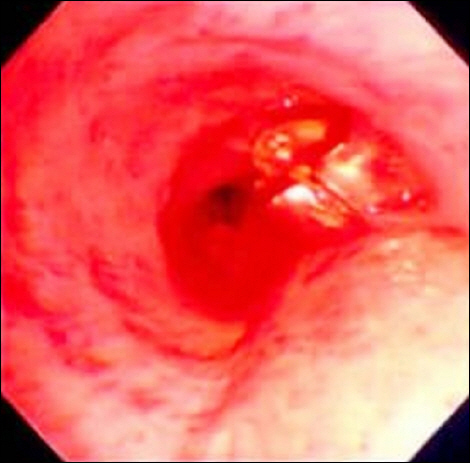
Fig. 2 Bronchoscope shows a metallic foreign body at the orifice of right upper lobar bronchus.

Fig. 3 Reusable grasping basket.
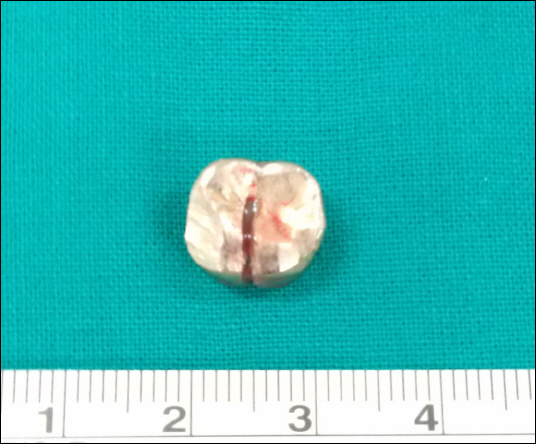
Fig. 4 The foreign body is 1.1 cm sized artificial tooth with crowning material.
Reference
-
1. Park SK, Cho EJ. Pneumonia from pulmonary aspiration of an antihypertensive anesthetic premedication. Anesth Pain Med. 2011; 6:402–5.2. Ramos MB, Fernández-Villar A, Rivo JE, Leiro V, García-Fontán E, Botana MI, et al. Extraction of airway foreign bodies in adults: experience from 1987–2008. Interact Cardiovasc Thorac Surg. 2009; 9:402–5. DOI: 10.1510/icvts.2009.207332. PMID: 19491125.
Article3. Huang PM, Kao MW. Endobronchial foreign body removed by flexible bronchoscopy using the trendelenburg position. Thorac Cardiovasc Surg. 2012; 60:545–7. PMID: 22207366.
Article4. Nussbaum E, Zagnoev M. Pediatric fiberoptic bronchoscopy with a laryngeal mask airway. Chest. 2001; 120:614–6. DOI: 10.1378/chest.120.2.614. PMID: 11502667.
Article5. Swanson KL, Prakash UB, Midthun DE, Edell ES, Utz JP, McDougall JC, et al. Flexible bronchoscopic management of airway foreign bodies in children. Chest. 2002; 121:1695–700. DOI: 10.1378/chest.121.5.1695. PMID: 12006464.
Article6. Swanson KL. Airway foreign bodies: what’s new? Semin Respir Crit Care Med. 2004; 25:405–11. DOI: 10.1055/s-2004-832713. PMID: 16088484.7. Dhanrajani PJ, Swaify GA. Aspiration of a bridge and a tooth. J Craniomaxillofac Surg. 1992; 20:91–2. DOI: 10.1016/S1010-5182(05)80474-3.
Article8. Knowles JE. Inhalation of dental plates—a hazard of radiolucent materials. J Laryngol Otol. 1991; 105:681–2. DOI: 10.1017/S0022215100117025. PMID: 1919331.
Article9. Svedström E, Puhakka H, Kero P. How accurate is chest radiography in the diagnosis of tracheobronchial foreign bodies in children? Pediatr Radiol. 1989; 19:520–2. DOI: 10.1007/BF02389562. PMID: 2797935.
Article10. Skoulakis CE, Doxas PG, Papadakis CE, Proimos E, Christodoulou P, Bizakis JG, et al. Bronchoscopy for foreign body removal in children. A review and analysis of 210 cases. Int J Pediatr Otorhinolaryngol. 2000; 53:143–8. DOI: 10.1016/S0165-5876(00)00324-4.
Article11. Levitan RM, Kinkle WC. Initial anatomic investigations of the I-gel airway: a novel supraglottic airway without inflatable cuff. Anaesthesia. 2005; 60:1022–6. DOI: 10.1111/j.1365-2044.2005.04258.x. PMID: 16179048.
Article12. Janakiraman C, Chethan DB, Wilkes AR, Stacey MR, Goodwin N. A randomised crossover trial comparing the i-gel supraglottic airway and classic laryngeal mask airway. Anaesthesia. 2009; 64:674–8. DOI: 10.1111/j.1365-2044.2009.05898.x. PMID: 19453322.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Removal of a Bronchial Foreign Body by Bronchoscopic Cryotherapy: A Case Study
- A Case of Removal of Pushpin by Flexible Bronchoscopy
- Awake supraglottic airway guided flexible bronchoscopic intubation in patients with anticipated difficult airways: a case series and narrative review
- Successful tracheal intubation using fiberoptic bronchoscope via an I-gel(TM) supraglottic airway in a pediatric patient with Goldenhar syndrome: A case report
- Removal of Sawdust Aspiration and Anesthetic Management: A case report
