Cancer Res Treat.
2014 Jul;46(3):317-321.
Case Report of Pulmonary Sarcoidosis Suspected to be Pulmonary Metastasis in a Patient with Breast Cancer
- Affiliations
-
- 1Division of Hematology/Oncology, Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea. cancer@korea.ac.kr
Abstract
- Standard endocrine therapy and chemotherapy can induce long-term remission in breast cancer patients; however, breast cancer can recur at any site. Pulmonary nodules with lymphadenopathy in advanced cancer patients are likely to be assumed as metastases. A 44-year-old woman with a history of breast cancer was presented to our institution with abnormal findings on 18-fluorodeoxyglucose positron emission tomography imaging, which suggested lung metastasis. She had previously been diagnosed with breast cancer (T1N2M0, Stage IIIa, intraductal carcinoma, triple negative cancer). Histological analysis of the mediastinal lymph node biopsy demonstrated sarcoidosis, showing a chronic, non-caseating, granulomatous inflammation. Our case highlights the need for non-malignant diagnoses in those with prior malignancies, and the need for histological evaluations in the event of first recurrence following potentially curative therapy.
MeSH Terms
Figure
-
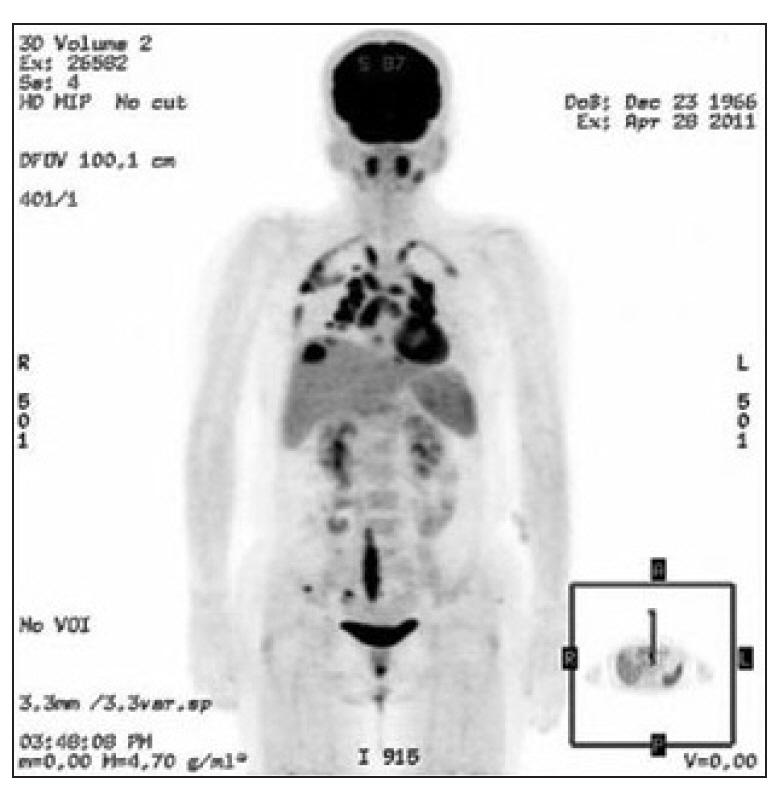
Fig. 1. Positron emission tomography-computed tomography scan of the patient. Multiple new hypermetabolic lesions were observed in the parenchyma of both lungs, both thoracic pleura, and multiple lymph nodes.
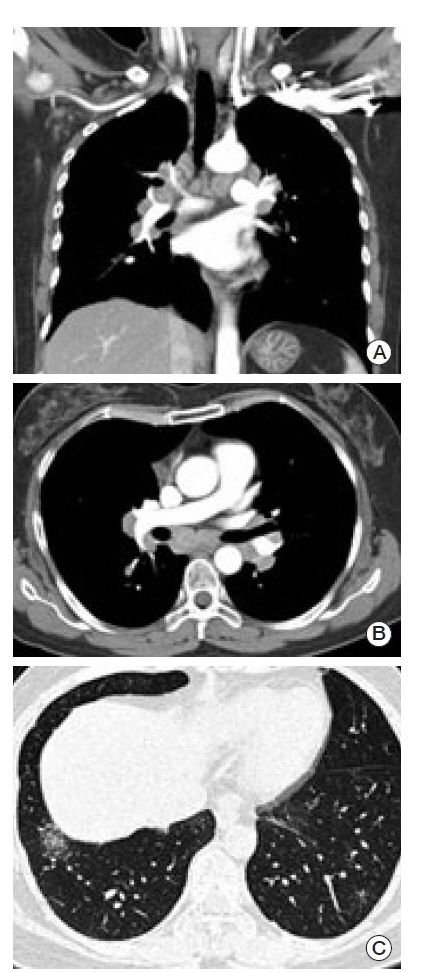
Fig. 2. Chest computed tomography scan. (A, B) Multiple lymphadenopathies were seen on both sagittal (A) and axial (B) sections in a mediastinal setting. (C) Faint ground-glass opacities and fine reticular densities were observed on both lower lungs. These findings were also observed on both upper subpleural lungs.
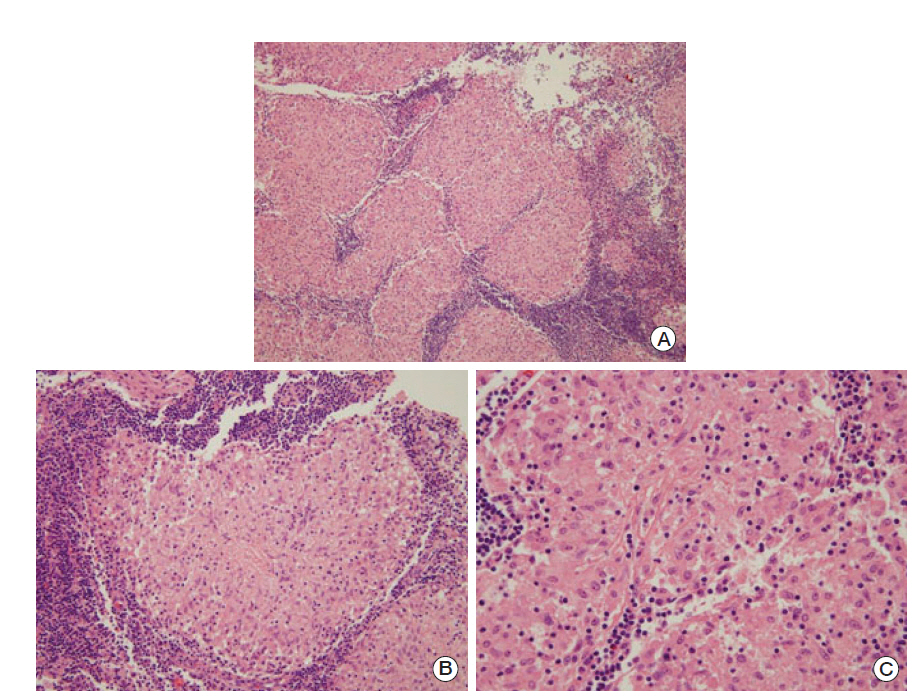
Fig. 3. Pathologic findings for the mediastinal lymph node tissue. Chronic non-caseating granulomatous inflammation was observed (H&E staining; A, ×100; B, ×200; C, ×400).
Reference
-
References
1. Simmons C, Miller N, Geddie W, Gianfelice D, Oldfield M, Dranitsaris G, et al. Does confirmatory tumor biopsy alter the management of breast cancer patients with distant metastases? Ann Oncol. 2009; 20:1499–504.
Article2. Reich JM, Mullooly JP, Johnson RE. Linkage analysis of malignancy- associated sarcoidosis. Chest. 1995; 107:605–13.3. Pennant M, Takwoingi Y, Pennant L, Davenport C, Fry-Smith A, Eisinga A, et al. A systematic review of positron emission tomography (PET) and positron emission tomography/computed tomography (PET/CT) for the diagnosis of breast cancer recurrence. Health Technol Assess. 2010; 14:1–103.
Article4. National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology. Fort Washington: National Comprehensive Cancer Network;2013.5. Karam M, Roberts-Klein S, Shet N, Chang J, Feustel P. Bilateral hilar foci on 18F-FDG PET scan in patients without lung cancer: variables associated with benign and malignant etiology. J Nucl Med. 2008; 49:1429–36.
Article6. Boyle P. Triple-negative breast cancer: epidemiological considerations and recommendations. Ann Oncol. 2012; 23(Suppl 6):vi7–12.
Article7. Askling J, Grunewald J, Eklund A, Hillerdal G, Ekbom A. Increased risk for cancer following sarcoidosis. Am J Respir Crit Care Med. 1999; 160(5 Pt 1):1668–72.
Article8. Reddy DJ, Sivaramakrishna G, Sarojini PS. Sarcoid-like lesion in regional lymph nodes of carcinoma breast. J Indian Med Assoc. 1959; 32:246.9. Giunti G, Mancini AM, Fontanili M. Sarcoidosis-like findings in the tributary lymph nodes of brease neoplasms. Arch Ital Anat Istol Patol. 1964; 38:19–46.10. Ataergin S, Arslan N, Ozet A, Ozguven MA. Abnormal 18FFDG uptake detected with positron emission tomography in a patient with breast cancer: a case of sarcoidosis and review of the literature. Case Rep Med. 2009; 2009:785047.
Article11. Dragoumis DM, Tsiftsoglou AP, Assimaki AS. Pulmonary sarcoidosis simulating metastatic breast cancer. J Cancer Res Ther. 2008; 4:134–6.
Article12. Gusakova I, Lavrenkov K, Ariad S, Mermershtain W. Pulmonary sarcoidosis mimicking metastases in breast cancer patients. Onkologie. 2007; 30:327–8.
Article13. Risbano MG, Groshong SD, Schwarz MI. Lung nodules in a woman with a history of breast cancer. Diagnosis: a sarcoidlike reaction in metastatic breast cancer. Chest. 2007; 132:1697–701.14. Brincker H, Wilbek E. The incidence of malignant tumours in patients with respiratory sarcoidosis. Br J Cancer. 1974; 29:247–51.
Article15. Romer FK, Hommelgaard P, Schou G. Sarcoidosis and cancer revisited: a long-term follow-up study of 555 Danish sarcoidosis patients. Eur Respir J. 1998; 12:906–12.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Abdominal Sarcoidosis Mimicking Peritoneal Carcinomatosis
- Port Site Metastasis of Breast Cancer after Video-Assisted Thoracic Surgery for Pulmonary Metastasis of Breast Cancer: A Case Report
- Roentgenological observation of pulmonary metastasis
- Subcutaneous Sarcoidosis of the Distal Lower Leg in a Middle-Aged Woman Associated with Pulmonary Sarcoidosis: a Case Report
- Lung Cancer Associated with Sarcoidosis: A case report
