Multiple Cardiac Metastases from a Nonfunctioning Pancreatic Neuroendocrine Tumor
- Affiliations
-
- 1Department of Internal Medicine, Chungbuk National University College of Medicine, Cheongju, Korea. sook3529@hanmail.net
- 2Department of Pathology, Chungbuk National University College of Medicine, Cheongju, Korea.
Abstract
- Pancreatic neuroendocrine tumors (pNETs) are rare neoplasms, which most commonly metastasize to the liver. However, intrathoracic metastases from pNETs are encountered infrequently. This report describes a case of nonfunctioning pNET with multiple cardiac metastases. A 56-year-old male presented with a palpable abdominal mass that showed progressive enlargement. Findings on computed tomography (CT) of the abdomen revealed two relatively well-marginated inhomogeneous low-attenuation masses, one in the head of the pancreas and the other in the tail. Multiple enhancing masses in the left pericardium with myocardial involvement were observed on chest CT and transthoracic echocardiography. Needle biopsies were performed on the mass in the tail of the pancreas and the left ventricular apical pericardium; histologic examination by hematoxylin and eosin morphology and immunohistochemical staining showed pNET in both. This is the first report of pNET with multiple cardiac metastases to previously undescribed metastatic sites.
MeSH Terms
Figure
-
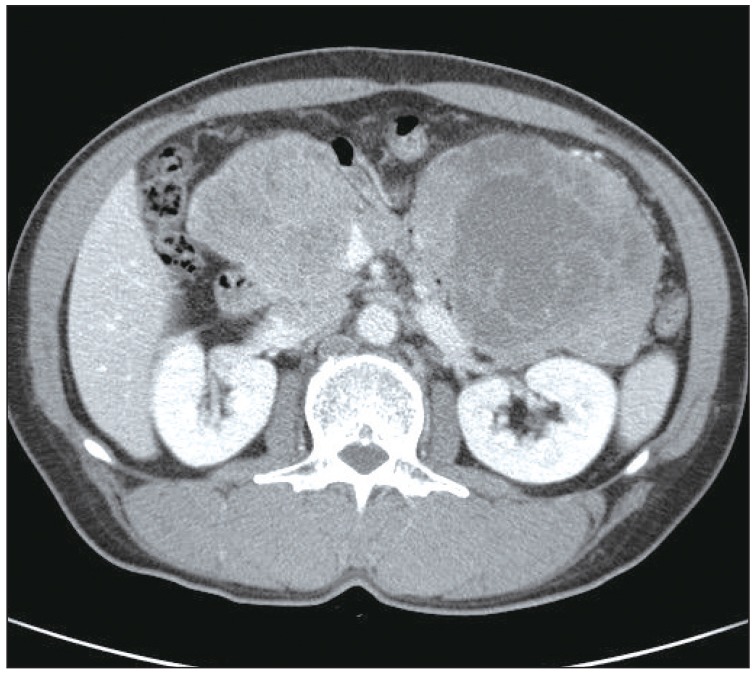
Fig. 1 Computed tomography (CT) of the abdomen. CT of the abdomen showed well-marginated enhancing large masses, one measuring 7.3×8.8 cm in the head of the pancreas and one measuring 12.0×9.2 cm in the tail.

Fig. 2 Computed tomography (CT) of the chest. Chest CT showed multiple enhancing masses distributed in the left pericardium.
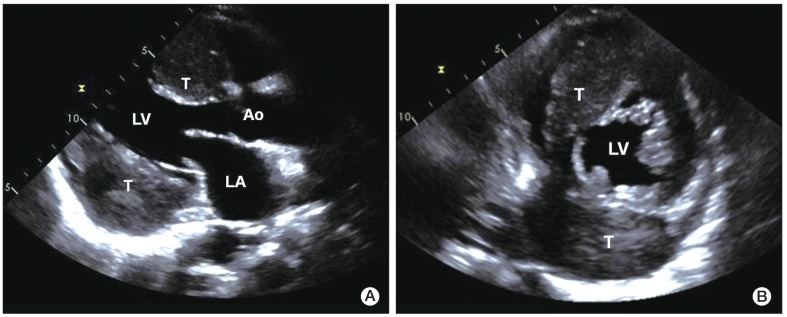
Fig. 3 Transthoracic two-dimensional echocardiography. Parasternal long axis view (A) and short axis view (B) showing heterogeneous round-shaped masses attached to the pericardium of the interatrial septal groove and the inferolateral wall of the left ventricle, with myocardial involvement. LA, left atrium; LV, left ventricle; Ao, aorta; T, tumor.
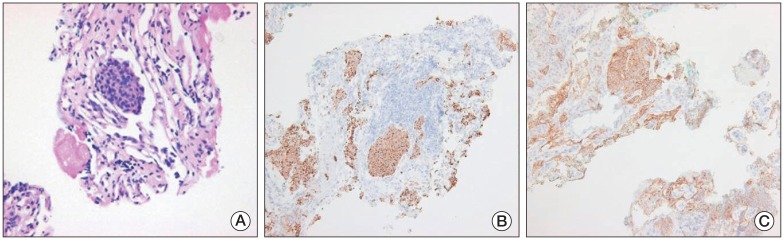
Fig. 4 Pathologic features of a needle biopsy of the mass in the pancreatic tail. (A) The tumor showed a nesting growth pattern with monotonous cells. The majority of tumor cells had a centrally located nucleus with moderate amounts of amphophilic cytoplasm. Nuclei were generally round to oval in shape, with coarsely clumped chromatin (H&E staining, ×400). Immunohistochemistry showed that the tumor cells were positive for chromogranin (B) and CD56 (C) (B and C, ×100).
Reference
-
1. Yao JC, Eisner MP, Leary C, Dagohoy C, Phan A, Rashid A, et al. Population-based study of islet cell carcinoma. Ann Surg Oncol. 2007; 14:3492–3500. PMID: 17896148.
Article2. Yao JC, Hassan M, Phan A, Dagohoy C, Leary C, Mares JE, et al. One hundred years after "carcinoid": epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol. 2008; 26:3063–3072. PMID: 18565894.
Article3. Halfdanarson TR, Rabe KG, Rubin J, Petersen GM. Pancreatic neuroendocrine tumors (PNETs): incidence, prognosis and recent trend toward improved survival. Ann Oncol. 2008; 19:1727–1733. PMID: 18515795.
Article4. Metz DC, Jensen RT. Gastrointestinal neuroendocrine tumors: pancreatic endocrine tumors. Gastroenterology. 2008; 135:1469–1492. PMID: 18703061.
Article5. Panzuto F, Nasoni S, Falconi M, Corleto VD, Capurso G, Cassetta S, et al. Prognostic factors and survival in endocrine tumor patients: comparison between gastrointestinal and pancreatic localization. Endocr Relat Cancer. 2005; 12:1083–1092. PMID: 16322345.
Article6. Hoffmann U, Globits S, Frank H. Cardiac and paracardiac masses: current opinion on diagnostic evaluation by magnetic resonance imaging. Eur Heart J. 1998; 19:553–563. PMID: 9597403.
Article7. Neragi-Miandoab S, Kim J, Vlahakes GJ. Malignant tumours of the heart: a review of tumour type, diagnosis and therapy. Clin Oncol (R Coll Radiol). 2007; 19:748–756. PMID: 17693068.
Article8. Bussani R, De-Giorgio F, Abbate A, Silvestri F. Cardiac metastases. J Clin Pathol. 2007; 60:27–34. PMID: 17098886.
Article9. Reynen K, Kockeritz U, Strasser RH. Metastases to the heart. Ann Oncol. 2004; 15:375–381. PMID: 14998838.
Article10. Moertel CG, Hanley JA, Johnson LA. Streptozocin alone compared with streptozocin plus fluorouracil in the treatment of advanced islet-cell carcinoma. N Engl J Med. 1980; 303:1189–1194. PMID: 6252466.
Article11. Moertel CG, Lefkopoulo M, Lipsitz S, Hahn RG, Klaassen D. Streptozocin-doxorubicin, streptozocin-fluorouracil or chlorozotocin in the treatment of advanced islet-cell carcinoma. N Engl J Med. 1992; 326:519–523. PMID: 1310159.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Nonfunctioning Neuroendocrine Tumor of the Pancreas in a 15-year-old Girl: a Case Report
- Transformation of Nonfunctioning Pancreatic Neuroendocrine Carcinoma Cells into Insulin Producing Cells after Treatment with Sunitinib
- Clinical and Immunohistochemical Characteristics of Pancreatic Neuroendocrine Tumor: Immunohistochemical Analysis of 7 Tumors
- Non-Functioning, Malignant Pancreatic Neuroendocrine Tumor in a 16-Year-old Boy: A Case Report
- Laparoscopic Enucleation of a Nonfunctioning Neuroendocrine Tumor of the Pancreas
