A Case of Idiopathic Hypereosinophilic Syndrome Presenting With Acute Respiratory Distress Syndrome
- Affiliations
-
- 1Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. leebj@skku.edu
- KMID: 2166956
- DOI: http://doi.org/10.4168/aair.2014.6.1.98
Abstract
- Although idiopathic hypereosinophilic syndrome(IHES) commonly involves the lung, it is rarely associated with acute respiratory distress syndrome (ARDS). Here we describe a case of IHES presented in conjunction with ARDS. A 37-year-old male visited the emergency department at Samsung Medical Center, Seoul, Korea, with a chief complaint of dyspnea. Blood tests showed profound peripheral eosinophilia and thrombocytopenia. Patchy areas of consolidation with ground-glass opacity were noticed in both lower lung zones on chest radiography. Rapid progression of dyspnea and hypoxia despite supplement of oxygen necessitated the use of mechanical ventilation. Eosinophilic airway inflammation was subsequently confirmed by bronchoalveolar lavage, leading to a diagnosis of IHES. High-dose corticosteroids were administered, resulting in a dramatic clinical response.
Keyword
MeSH Terms
-
Adrenal Cortex Hormones
Adult
Anoxia
Bronchoalveolar Lavage
Diagnosis
Dyspnea
Emergency Service, Hospital
Eosinophilia
Eosinophils
Hematologic Tests
Humans
Hypereosinophilic Syndrome*
Inflammation
Korea
Lung
Male
Oxygen
Pulmonary Embolism
Radiography
Respiration, Artificial
Respiratory Distress Syndrome, Adult*
Seoul
Thorax
Thrombocytopenia
Adrenal Cortex Hormones
Oxygen
Figure
-
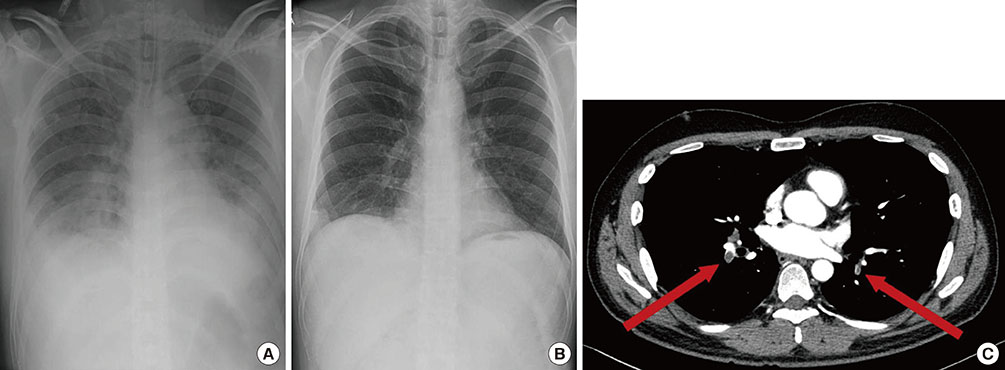
Fig. 1 (A) Patchy areas of consolidation with ground-glass opacity are observed in both lower lung zones on the initial chest radiograph. (B) Follow-up chest radiograph on hospital day 9 shows a dramatic decrease of lung infiltrate. (C) Chest CT scan shows bilateral acute pulmonary thromboembolism (arrows) involving both pulmonary arteries.

Fig. 2 Skin biopsy of the purpuric lesions of the right ankle shows (A) diffuse eosinophilic perivascular infiltration in the dermis and (B) eosinophilic abscess in the subcutaneous fat (H&E stain, ×40 magnification).
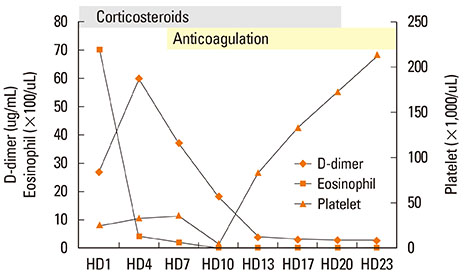
Fig. 3 Platelet counts, eosinophil counts, and D-dimer levels during hospitalization. Following initiation of high-dose corticosteroid therapy, eosinophil counts decreased to normal levels by day 3, and platelet counts progressively recovered. D-dimer levels initially elevated, but began to decrease with anticoagulant therapy. HD, hospital day.
Cited by 1 articles
-
Chronic eosinophilic leukemia with a
FIP1L1-PDGFRA rearrangement: Two case reports and a review of Korean cases
Sang-Yong Shin, Chul-Won Jung, Dong-Chull Choi, Byung-Jae Lee, Hee-Jin Kim, Sun-Hee Kim
Blood Res. 2015;50(1):58-61. doi: 10.5045/br.2015.50.1.58.
Reference
-
1. Klion A. Hypereosinophilic syndrome: current approach to diagnosis and treatment. Annu Rev Med. 2009; 60:293–306.2. Fauci AS, Harley JB, Roberts WC, Ferrans VJ, Gralnick HR, Bjornson BH. NIH conference. The idiopathic hypereosinophilic syndrome. Clinical, pathophysiologic, and therapeutic considerations. Ann Intern Med. 1982; 97:78–92.3. Spry CJ, Davies J, Tai PC, Olsen EG, Oakley CM, Goodwin JF. Clinical features of fifteen patients with the hypereosinophilic syndrome. Q J Med. 1983; 52:1–22.4. Roufosse F, Goldman M, Cogan E. Hypereosinophilic syndrome: lymphoproliferative and myeloproliferative variants. Semin Respir Crit Care Med. 2006; 27:158–170.5. Winn RE, Kollef MH, Meyer JI. Pulmonary involvement in the hypereosinophilic syndrome. Chest. 1994; 105:656–660.6. Chusid MJ, Dale DC, West BC, Wolff SM. The hypereosinophilic syndrome: analysis of fourteen cases with review of the literature. Medicine (Baltimore). 1975; 54:1–27.7. Simon HU, Rothenberg ME, Bochner BS, Weller PF, Wardlaw AJ, Wechsler ME, Rosenwasser LJ, Roufosse F, Gleich GJ, Klion AD. Refining the definition of hypereosinophilic syndrome. J Allergy Clin Immunol. 2010; 126:45–49.8. Dulohery MM, Patel RR, Schneider F, Ryu JH. Lung involvement in hypereosinophilic syndromes. Respir Med. 2011; 105:114–121.9. ARDS Definition Task Force. Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, Camporota L, Slutsky AS. Acute respiratory distress syndrome: the Berlin definition. JAMA. 2012; 307:2526–2533.10. Pepe PE, Potkin RT, Reus DH, Hudson LD, Carrico CJ. Clinical predictors of the adult respiratory distress syndrome. Am J Surg. 1982; 144:124–130.11. Hudson LD, Milberg JA, Anardi D, Maunder RJ. Clinical risks for development of the acute respiratory distress syndrome. Am J Respir Crit Care Med. 1995; 151:293–301.12. Fowler AA, Hamman RF, Good JT, Benson KN, Baird M, Eberle DJ, Petty TL, Hyers TM. Adult respiratory distress syndrome: risk with common predispositions. Ann Intern Med. 1983; 98:593–597.13. Villar J, Blanco J, Añón JM, Santos-Bouza A, Blanch L, Ambrós A, Gandía F, Carriedo D, Mosteiro F, Basaldúa S, Fernández RL, Kacmarek RM. ALIEN Network. The ALIEN study: incidence and outcome of acute respiratory distress syndrome in the era of lung protective ventilation. Intensive Care Med. 2011; 37:1932–1941.14. Doyle RL, Szaflarski N, Modin GW, Wiener-Kronish JP, Matthay MA. Identification of patients with acute lung injury. Predictors of mortality. Am J Respir Crit Care Med. 1995; 152:1818–1824.15. Ogbogu PU, Rosing DR, Horne MK 3rd. Cardiovascular manifestations of hypereosinophilic syndromes. Immunol Allergy Clin North Am. 2007; 27:457–475.16. Park YM, Bochner BS. Eosinophil survival and apoptosis in health and disease. Allergy Asthma Immunol Res. 2010; 2:87–101.17. Ogbogu PU, Bochner BS, Butterfield JH, Gleich GJ, Huss-Marp J, Kahn JE, Leiferman KM, Nutman TB, Pfab F, Ring J, Rothenberg ME, Roufosse F, Sajous MH, Sheikh J, Simon D, Simon HU, Stein ML, Wardlaw A, Weller PF, Klion AD. Hypereosinophilic syndrome: a multicenter, retrospective analysis of clinical characteristics and response to therapy. J Allergy Clin Immunol. 2009; 124:1319–1325.e3.18. Park SM, Park JW, Kim SM, Koo EH, Lee JY, Lee CS, Choi DC, Lee BJ. A case of hypereosinophilic syndrome presenting with multiorgan infarctions associated with disseminated intravascular coagulation. Allergy Asthma Immunol Res. 2012; 4:161–164.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anesthetic Management of a Patient with Idiopathic Hypereosinophilic Syndrome: A case report
- A Case of Hypereosinophilic Syndrome
- A Case of Idiopathic Hypereosinophilic Syndrome Presenting Acute Pulmonary Edema
- A case of idiopathic hypereosinophilic syndrome presenting multiple organ injuries with eyeball involvement
- Idiopathic Hypereosinophilic Syndrome Involving Thoracic Spine
